Dalal.Holdings
-
Posts
6,339 -
Joined
-
Last visited
-
Days Won
2
Content Type
Profiles
Forums
Events
Everything posted by Dalal.Holdings
-
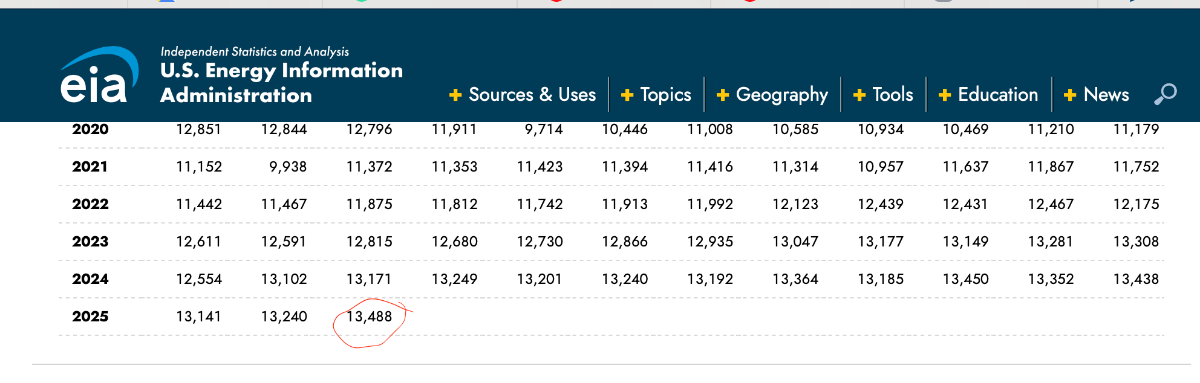
You have all time high U.S. production at the same time OPEC is flooding & China transitioning its auto industry from gasoline… People in the oil patch can say “rigs are down” or “production is going down” or “just wait a few more months” all they want. I don’t care what they’re saying. Only what they’re doing.
-
Very Intelligent move from European regulators if true. Not only do the governments own significant stakes in many of the firms, but they also fund them and are desperate for these firms to become true champions. Great idea to hobble the firms just while they are getting going. Only super smart Euro regulators come up with "special taxes" on their best performing sectors. These are very intelligent people who wear ties and ride bicycles to work and were educated at "the best" universities. They also helped come up with amazing innovations like the AI Act and GDPR. True geniuses.
-
Oil bulls every time: "production is coming down", Reality:

-
What do you mean though? Russia has installed advanced Tire Anti-Drone System on its planes (albeit the # of tires has come down over the years):
-
-
“No new production added” [citation needed] Here’s my citation: https://www.eia.gov/dnav/pet/hist/leafhandler.ashx?n=pet&s=mcrfpus2&f=m Lol, U.S. production at all time highs…
-
I don’t care about what they are saying. Only what they are doing.
-
"Production is coming down" "Below the cost of production" So many claims with no real citations or evidence
-
Yeah except that’s not what I said at all. No point in discussing further.
-
Not only is the U.S. fiscally challenged vs say Germany, but U.S. equities are much more expensive than European counterparts. There has been good reason for that as the Eurozone (esp Germany) has been in multi-year economic stagnation due to self imposed austerity. My bet is that changes in the coming years.
-
As I said, I hope @wabuffo is right and the alarmists wrong. However, hope is not a strategy. I'll continue owning some Euro denominated assets and avoid long duration dollar denominated bonds.
-
How about Stan Druckenmiller? Is macro not in his circle of competence either ? https://www.cnbc.com/2023/11/01/stanley-druckenmiller-says-government-needs-to-stop-spending-like-drunken-sailors-cut-entitlements.html https://www.bloomberg.com/news/articles/2023-05-02/druckenmiller-warns-us-debt-crisis-worse-than-he-imagined https://grafa.com/news/cryptocurrencies-stanley-druckenmiller-warns-of-us-debt-crisis-308016
-
I'm curious though--on one hand you have Warren Buffett and Jamie Dimon being "alarmist" about the unprecedented U.S. fiscal situation and on the other you have @wabuffo saying not to worry and it's the roaring 20's all over again. It seems the board has gone with the latter instead of the former two individuals... We'll see who's right, I guess. (Of course, I hope @Wabuffo is right and we prosper, but hope is not a viable strategy for me)
-
Even if Jamie is being alarmist, it's probably a good thing because he knows exactly who is listening whenever he opens his mouth: https://www.wsj.com/livecoverage/stock-market-trump-tariffs-trade-war-04-09-25/card/trump-watched-dimon-interview-on-fox-before-deciding-on-tariff-pause-3xJmTRvWCOLsnvsmAJwL?gaa_at=eafs&gaa_n=ASWzDAhVJQNmG54YIa9zQOc-yT-m9vTPJ9TPytI6wbZBxIb1tuLvmRzJDx17mNPsDes%3D&gaa_ts=683b42ea&gaa_sig=urualXYipkFj-5wJZfEqUgbhmlDpvbIWK8xluGSUcgtHZLwYf3PVi1vRtBc-67HPc5-x2N5IDtVPDlaD796C4g%3D%3D https://www.independent.co.uk/news/world/americas/us-politics/chase-bank-ceo-recession-trump-interview-b2730383.html
-
https://www.wsj.com/finance/jpmorgans-jamie-dimon-predicts-crack-in-the-bond-market-citing-u-s-fiscal-mess-9d90cb3f?mod=hp_lead_pos1
-
The problem is that +/- 200Bps is not symmetric in probability terms. Interest rates can only go down to zero (or slightly negative), so there is a hard lower limit. Meanwhile, there is no real upper limit (rates peaked around 18-20% in early 1980s, which is +1300 bp from now--meanwhile, interest rates will never go -1300 from where we are today to -9%, so there is a clear asymmetry). Furthermore, if the currency you are earning interest in is devalued, you need to subtract that from your returns. If you hold equities or some other asset in that currency, at least it will appreciate in proportion to the currency devaluation, but the bonds will not (if you are a borrower via a mortgage though, the price of the house securing it appreciates with currency devaluation (and you get levered upside on your equity stake) while the mortgage remains fixed which is why a mortgage is a great instrument for the borrower in this scenario and terrible for the lender).
-
I think the German and Japanese defense ecosystems are set to undergo rapid change as the Post-WW2 framework ends
-
Even Subaru makes some military helicopters -- Subaru !
-
Cash is trash...until there's a bear market, of course. Then, those who hold cash (or ST bonds) can scoop up distressed assets at distressed prices as Warren has demonstrated many times during his career. That's why he has alpha and so many don't. Those who were all-in at the top get to ride the bear market all the way down and maybe watch everything they own get cut in half. If they were levered, the damage is much worse. Either way, this is the bonds thread. While T-bills might provide "subpar" returns of 4.2%, 30 year treasury bonds provide a whopping ~5% return for locking your money in for 30 years while taking on massive interest rate risk. I'm sure those extra 80 bp of yield will be worth it...good luck to those who think that's a good deal. I know Warren doesn't and neither do I. Contrary to those who are buying 20, 30 year bonds, I'm taking the opposite position: I still have 26 years left on my mortgage. If the dollar crumbles, a 30 yr fixed mortgage becomes a great position to be in while a 30 year fixed bond an equally atrocious position. Default risk is irrelevant. Act accordingly.
-
Anyone got any interesting Japanese defense co's/suppliers ?
-
He's not paying anything, he's getting paid. And it's very short term parking (not long term parking) whereby he has the optionality to quickly dump the T-bills and move onto something else. And note--he's also been dumping BAC which has long duration assets on its books.
-
He's only in short term T-bills, notably refuses to go out in duration to get an extra 80 bps of yield unlike some folks
-
https://finance.yahoo.com/news/warren-buffett-big-worry-over-161500718.html Wonder why Warren save this theme for his very last AGM... Bah, I'm sure it's nothing
-
I've been in Europe for a while, but I want to buy more. I'd like the German government to get its act together and pass a budget that actually spends on infra and defense and pushes the country out of its multi-year stagnation. It seems Merz realizes this is the last chance for the mainstream to act (otherwise AfD will win the next set of elections). There ought to be a sense of urgency then... However, the first vote for chancellor that failed was not reassuring as it indicates that there are some holdouts in the mainstream parties in Bundestag that may thwart the aggressive action Germany needs. And of course Merz has promised not to form a coalition with AfD members, so that leaves few options if he can't get votes from his own coalition... Unfortunately, being decisive is not something Europe has had going for it for a long time, perhaps least of all Germany... Germany is the only country in the West with the fiscal space to do something big and meaningful. They'd better act with a sense of urgency
-
Given Trump's repeated "Dollar is too strong" statements, it's hard to be surprised by this, similar to oil bulls being rug pulled on oil prices coming down when Trump/Bessent made clear low oil prices are v important to them. A weak dollar is like another layer of Tariffs on all imports in that it makes imports more expensive. It does boost exports (and the reported dollar profits of multinationals that do business in other currencies). As an American investor though, the play was to use strong dollars to purchase overseas assets, especially when the USD was at multiyear highs at the beginning of the year on the eve of the inauguration of this administration (the Euro was near USD parity). Hence, YTD performance matters in this case. Ironically, up until this year, the mantra was "Live in Europe, invest in America"...some of us did the exact opposite.