Cigarbutt
-
Posts
3,473 -
Joined
-
Last visited
-
Days Won
1
Content Type
Profiles
Forums
Events
Everything posted by Cigarbutt
-
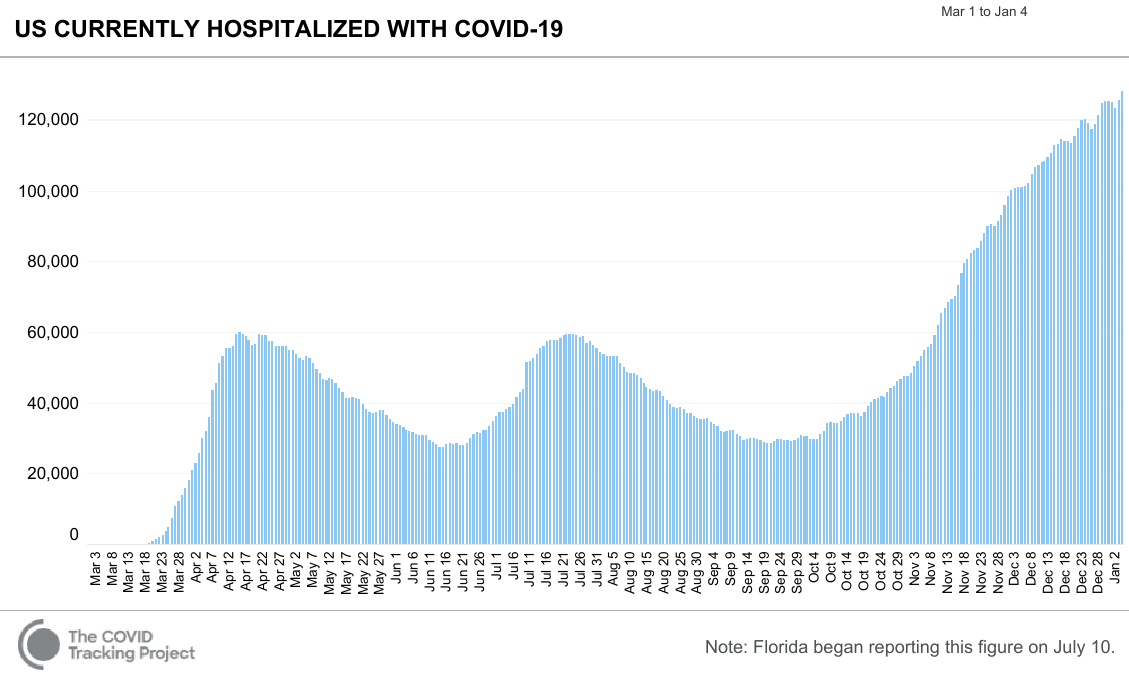
^Of course scrutiny is warranted in all directions. This distribution logistics challenge is an opportunity for healthy competition: https://covid19tracker.ca/vaccinationtracker.html https://www.nbcnews.com/health/health-news/map-covid-19-vaccination-tracker-across-u-s-n1252085 https://ourworldindata.org/grapher/covid-vaccination-doses-per-capita?tab=chart&stackMode=absolute&time=earliest..latest®ion=World May the best win! As far as Christmas day, 'Boxing Day' and New Year's day as well (to some extent), i don't have enough granular knowledge for a definitive opinion, especially a disparaging one, but it appears that many people with decision power underestimated the capacity of some workers to contribute to the effort on those specific days. However, it also seems that many hospitals and nursing homes really have a hard time with human resources (tired, sick etc). i know many people who work in hospitals and homes where community spread is still rampant and many have been recently told to cancel any planned holidays for the next few weeks. These people come home at the end of their day, turn on the TV and see sports bloggers turned data analysts at the airport waiting to fly to their all-included let's party adventure. There is a disconnect between what is happening in the real world (hospital beds etc) and what some people think is happening. Also, the Christmas day lull seems to be a national phenomenon which does not justify the delay but may contribute to understand, at least partially, some of the inputs that went into the decision making process.

-
Hmm.. Difficult era for compromises. On the one hand, you have people suggesting that vaccines should have obviously been given in early 2020 and "they" lacked courage (professional and personal), integrity or even intellect. On the other hand, you have people suggesting that vaccines are, as of now, dangerous and guinea-pig products and "they" are hysterical incompetents (at best) or fanatical conspiration partisans with a Machiavellian plan. What is confusing is that the same people seem to consistently reach similar contaminated conclusions about many topics and (needed assumption for coherence) "they" must manifest some kind of personal dissociation disorder. At times, it must be tough to be "they". Rumor has it that a clerical staff person in medical records was able to jump queue and get the vaccine. Conclusion?: the whole process is a disgrace.
-
^The logistics are being defined as 'we' go and there could be many explanations for the developing age distribution. The average age of healthcare workers is about 40 and about a third are 50+, at large. Anecdotal experience suggests that frontline workers in "busy" areas tend to be younger. It seems also the age profile has gotten younger during the pandemic in "hot" areas due to turnover according to risk factors.
-
Are (specific) discussions bound to evolve that way? The answer, from a purely individual perspective, is that there is no benefit now (scarcity) and later. The answer though can become more complicated. Read the following if you have 3 minutes even if it's 'scientific' and even if some uncertain hypotheses are thrown around. https://www.realclearscience.com/articles/2020/12/21/why_did_reindeer_in_norway_eat_each_others_antlers_653829.html From a purely individual perspective, the reindeer's best course of action is to enter into destructive behavior (both at the individual and collective levels). From an evolutionary standpoint, the right outcome is happening. i wonder if humans would have been able to deal with a similar challenge, given the inherent and baffling way to somehow be able to collaborate and cooperate? Happy New Year to you. Individual opinion: The best thing about humans is that "they" have emotions.
-
The distribution plan in IL and Chicago is similar to what is being done elsewhere. For the initial week, "they" chose to prioritize regional "hub" hospitals where prevalence has been high (the candidates there include frontline healthcare workers). Early distribution plans also include nursing homes (residents and at-risk staff) and first-line responders. Over time, it can be assumed that the age profile will skew higher.
-
Didn't Mr. 'Chuck' Prince say something similar, at some point along the way? I didn't say that there will be no effects from Fed actions. The Fed is obviously doing what is doing because it wants to obtain some effects, not because it's bored. All I was saying is that if the Fed wants to lower long term rates it is totally in its power to do it. Fair enough. It just seems the Fed is bound to do more of the same at every turn without retaining the ability to eliminate policies once 'acute' phases quiet down. wabuffo uses a digging hole analogy (a concept i agree with) and one has to hope that the music doesn't stop. There is a there-is-no-alternative flavor and it feels awkward? Some people suggest that the Dunning-Kruger effect is most at risk with noobs like me and with 'experts' so i wonder?
-
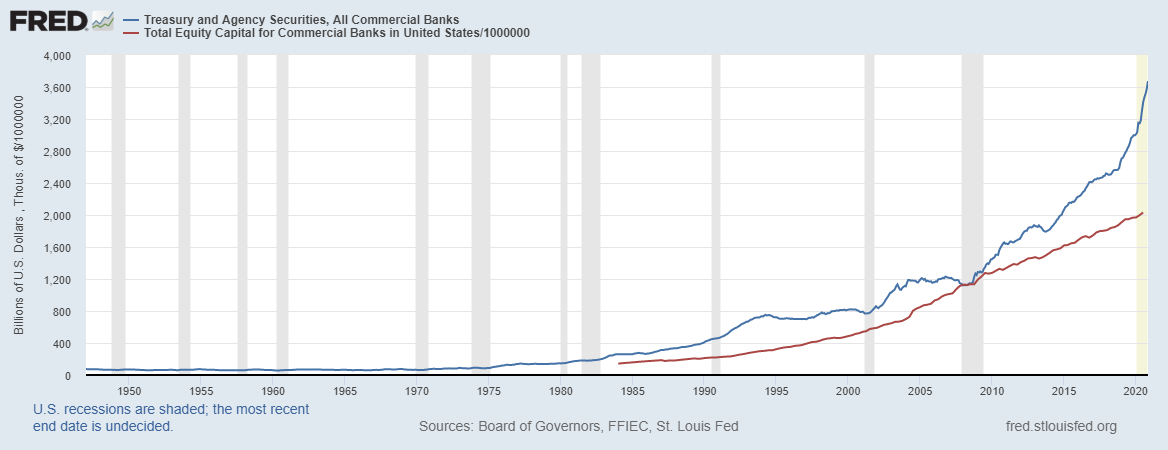
The idea here is to avoid circular arguments, falling in rabbit holes or drifting in ####### discussions. BTW, Have a great 2021. In a way, because of various capital and regulatory rules, it's not only excess reserves that have been forced upon commercial banks, it's also the treasury and agency 'paper' which has been supplied generously lately (some would say exponentially). As of end 2019, only for the government paper, pre-covid... Attached is a graph adjusted for size comparison indicating that commercial banks have been forced-fed some stuff that they perhaps could do without but i seem to remember that you reject the notion of crowding out (public debt displacing private investments). FWIW, i've deeply studied the Weimar episode from various angles. TL;DR: The inflation story is fascinating but 'we, haven't crossed that bridge (yet) and if we do, it's not the rise in the money supply that we'll need to worry about. ---)Back to does the fed control interest rates: it does until it no longer does (non-linear)
-
From anecdotal to fundamental and back to sentimental Anecdotal Real estate market movements in my street reflect (somewhat muted though) general trends in Canada. Echoing Viking’s anecdotal stuff, our next-door neighbor moved about 300 feet to the other side of the street in order to buy the second most expensive house of the area. In Canada, refinancing is not so easy and the transaction helped in achieving a net positive development for paper worth (and short term liquidity). They have two very young children and, the other day, during typical neighbor chit-chat, the topic of funding higher education was touched upon but rapidly switched to the large spa that they plan to acquire next summer. Keeping the house is contingent on both keeping their jobs and they have a margin of safety based on the value of their two leased cars. (Note: they sold their house practically the same day it was listed with a very optimistic list price and with the winning price above and with the buy decision made essentially after a virtual visit; what’s not to like?) Fundamental An argument can be built that Canada real estate prices are absurd but obviously everything depends on the eye of the beholder. Historically, various factors are mentioned (vibrant work market, healthy influx of immigrants inhabited by a strong propensity for homeownership and various supply issues). Some also mention the central role of various public support tools and the incredibly low interest rate reign. Well, in 2020, job losses was the order of the day but various interventions to support incomes and deferral payment schemes were supplied. And immigration flux decreased by about 50% (due to various administrative delays in the supply chain) but the BoC (and a freshly minted QE program) came to the rescue. The 2021 central debt issue plan hasn’t been fully internalized yet but another 300B is the base case scenario if one reads between the lines but who cares (now)? The overriding factor is sentiment and how do you assess that, in terms of sustainability? From page 8 of the pdf document, over the course of human events in 2020: “Among non-homeowners, the expectation of buying in the next year has more than tripled, from 7% at the end of last year to 14% in the first wave of the survey, 16% in the second wave, 19% in the third wave and 23% in the fourth wave.” The dream lives on and more. https://www.bankofcanada.ca/stats/cars/results/bd_auction_schedule.html It looks like the GoC is aiming to lengthen duration. Who could blame them at this point? https://mortgageproscan.ca/docs/default-source/consumer-reports/rapidly-evolving-expectations-in-the-housing-market---december-2020-en.pdf Sentimental Just a few weeks ago, I spotted a few properties (with the goal to move into one and own a few residential apartment properties) and actually completed due diligence (to the extent possible). The catch is that those properties are not on sale (yet). i bet they will.
-
Didn't Mr. 'Chuck' Prince say something similar, at some point along the way?
-
During 2020 (‘recession’ period), the Case-Shiller house price index went up by almost 10% (!). Why? For many reasons and (very) low interest rates? Isn’t the Fed driving interest rates down? Share of the Fed-held agency MBS vs total agency MBS (%) Before 2009: 0% 2010: 15% 2012: 13% 2014: 24% 2016: 23% 2018: 20% (attempt at ‘tapering’ and in 2019, withdrawal tantrums) 2019: 16% end 2020: about 23% (in 2020, there was record MBS issuance, re-fi activity and Fed involvement) Isn’t the Fed an essential player here even if only a swapper? In early March, their extra involvement was key to restore the volatility in spread that happened in the agency MBS market but the market has become habituated to their long-term ‘involvement’. Opinion: Like the Eagles song, the Fed can check out anytime but can never leave. The 30-yr mortgage rate is influenced by the effective Fed fund rate and is tightly correlated to inflation. If you know where inflation is going, you know where the 30-yr mortgage rate is going. Note: crossing zero though is mostly uncharted territory.
-
i just spent a few short minutes reviewing what you posted and will reply in short form. -The vitamin question C question was because a champion of various alternative treatments, that you often refer to, used to (in the spring) suggest this was a miracle treatment. It seems the miracle has transmogrified. -i don't follow zinc-supplement regulations that closely and my only relevant experience is when someone recently tried to sell me a radon detector for my basement (read about it, it's interesting). When i asked for independent thought time, the person suggested a zinc supplement as an alternative. And then i wondered. -The ivermectin stuff is interesting. The MD in France who is the lead investigator is specialized in skin disease (and skin manifestations of sexually transmitted diseases) and has an interest in scabies (and automatically ivermectin; careful here: everything may look like a nail). She (et al) appears to be reasonable. i'm not sure why ivermectin has not been more studied and there may be some inertia from pharma for various reasons including limited profit potential but i don't see a material conspiracy. There are reasons why it could work and there are major reasons why it may not and the recommendation to go over and above observational and anecdotal evidence applies. As an aside, i was able to watch and listen to two short presentations of potential skin manifestations of covid since last April (dermatology). In the first one, many ideas were submitted (correlation) and, in the second, most correlated findings were simply that, correlated. Peer review can be a pain for career advancement. -The youtube person is a dentist (who may have a vitiligo problem to attend to). Still, one has to hear (and analyze) what she says. She refers to anecdotal evidence for ivermectin. --- @Gregmal You may have noticed that this board has been drifting (to where?). It looks like removing the political threads may be a step in the right direction. Over time, i try to improve. How? By trying to include necessary and relevant information (room for improvement there). i wonder if it's worth trying to contribute in a way as to maintain the constructive aspect. However, i've become convinced that our respective senses of humor are not quite compatible (in most cases). Making friends in this competitive forum can only be an unexpected side effect. Near graduation, a mentor (i did not realize it then) expressed that first, you have to competent. What's second? It's up to you to figure out, he said. (people said he had been a real jerk at some point but he was hit by a nasty disease and then he asked to teach the ethics class) --- @boilermaker75 i'm about to send you a private message.
-
You're obviously trolling once again and maybe you're looking for some entertainment so, just for fun: what is the problem if there is no problem? For those looking for a more balanced take in this distribution challenge: https://www.ft.com/content/a1bb5262-0628-401b-b5cc-66a64c17130b (note: i'm busy today and don't plan to argue here. My second child is turning 23 today and am responsible for some of the planning; she's beautiful, gifted, graduating as an engineer this year, has a bright future and is quite liberal but hey! nobody's perfect.)
-
Disclosure #1: stock picking is the way to go, if you can. So, this is likely a waste of time. Disclosure #2: i've been 'communicating' with various 'friends' and acquaintances for holiday greetings and when the discussion superficially touches investments, i feel relatively stupid and got to watch out for envy and maybe accept the real possibility of stupidity (relative or absolute). ----- I never thought Mr. Mandelbrot would be mentioned here and there you go. When i graduated in 1996 (mostly science-related), i decided to 'manage' household investments and had to learn what an asset was. For a year or two, went through 'economics' and came across Mr. Mandelbrot's writings. Fascinating. He was a remarkable individual, perhaps from the same multi-dimensional mold as Mr. Charlie Munger. Three things stuck from the unique thinker. First, contrarianism. From the source: "As I allowed myself to drift, I soon came to view the normal unpredictability in life as contributing layers or strata of experience that are valuable, demand no apology, and add up to a unique combination." Second, conceptual tools when i met annual reports from Mr. Prem Watsa somewhere in early 1997. That's when 'value investing' came to view. Understanding FFH then meant to understand the value of reserves (wild euphemism in this case) and i realized that not many people really looked at reserve triangles. Mr. Mandelbrot's ideas of mixing deterministic and stochastic models were very helpful then, and periodically after. Third, how to deal with physics envy in softer fields or how to mix chaos to models (tensile strength and fractures, weather 'prediction', inverting yield curves etc). Of course, the inverting yield curves and ultra-low interest rates are saying something. And the wildness of the message lies in wait. It feels like the whole covid thing was simply an interlude. ----- Still, by using a variety of historical measures, this market (valuation, spreads etc) is the most optimistic it has ever been. Of course, the market could be right and it's really a great time to be alive.
-
Trying to adjust along the way involved improvisation at times and the risk of uncomfortable incongruities. i can't speak for NY, but people in my area seemed to be motivated by good intentions, whatever that means. It looks like NY has made some adjustments. If one can't take a dump where they want, what kind of country is this? https://www.pix11.com/news/coronavirus/ny-backtracks-on-restaurant-bathroom-ban-amid-new-outdoor-dining-restrictions It looks like most constructive energy should be devoted to vaccine distribution even if 99.999% of people survive the false positive tests but the toilet question has been one of the rare topics where Mr. Cuomo needed 'expert' assistance. To lid or not to lid, that is the question. Putting sanitary questions out of the way, i wonder if Mr. Buffett (in one of of his very rare public appearances) is not on the right track when he recently suggested that the PPP program should be maintained, adjusted, improved in order to build a bridge to the light at the end of the tunnel for some of the most obvious collateral damage.
-
^One has to decide if it's worthwhile to listen and watch also. One has to wonder what Mr. Munger thought of the interviewer. He was unusually warm (for a few short seconds) at the conclusion. These days, one has to wonder also if this is/was his last interview. He is truly a fascinating person. What did he mean by: "I think we’re very near the edge of playing with fire."? ?
-
A more reader-friendly version. https://www.rev.com/blog/transcripts/investor-charlie-munger-caltech-interview-transcript-december-16
-
https://www.ft.com/content/2b41c6cb-ba68-47c7-b488-7bf778d64050 Download at your own peril.
-
Thanks for the link. The author covers many aspects and the perspective is interesting although debatable for some parts. Along similar lines: https://vitals.lifehacker.com/how-they-made-a-vaccine-so-fast-1845880519
-
... who's going to pay for all this? MMT means we pay it forward. Again, you are right on target. Still, who is we? (This may be a nagging question for a while) In a way, (forget the white supremacist symbol on the megaphone for a minute) that's what the gym owner is trying to figure out when saying: we will not be backing down. -----)back to the virus, investment implications and all..
-
Interesting perspective, as always. (?) It's difficult to build on this from an analysis or investment point of view but there's the following question: who's going to pay for all this? The answer (which has been wrong so far) has been increased taxation but what the fukk do i know? http://www.haver.com/comment/201214z.png http://www.yardeni.com/pub/tc_20201209_4.png @investor20 Any update on vitamin C?
-
Maybe a way to conceptualize these 'financing' deals with OMERS et al is to see them like quasi-perpetual preferred equity contracts. The coupon rate is relatively high but allowed FFH to acquire large controlling pieces of great businesses and it looks like they can decide, periodically, to buy back the financing at par value and not according to book value. It can be a win-win proposition.
-
@cwericb Last night, a few minutes before 8PM, a large UPS cargo plane landed about 20 km from where i live. Some people even went there to see the plane land. And now the vaccine is spreading like a virus. ----- If interested in vaccine distribution: https://www.kff.org/coronavirus-covid-19/event/dec-3-web-briefing-what-happens-once-there-is-a-covid-19-vaccine-key-challenges-to-vaccinating-america/ https://www.msn.com/en-ca/news/us/they-re-not-just-treating-covid-rural-area-doctors-are-fighting-vaccine-distrust/ar-BB1bSWAp?ocid=msedgntp The second link is about the ‘narrative’ that occurs where real people live in the ‘periphery’. There is a difference between anti-vaxx and hesitancy and it looks like more effective vaccine coverage can be obtained in leading by example in order to alleviate hesitations. The first link is relatively long but slides can be downloaded and looked at for a few seconds to get the gist. Two messages: 1-the distribution will be a challenge for many reasons (logistics and others) partly because of heterogeneity in regional plans. 2-the areas (trend, not all) that report the highest ‘casualty’ from the virus are also the least prepared for distribution and are also where people show the most ‘hesitancy’. There’s work to be done. The vaccine story concerning procurement and distribution is 100%-owned by central “authorities”, which should be a default option but it’s still an opportunity to build back trust. During this outbreak, there was a lot of unnecessary denial: unusual focus on ‘alternative’ theories and their proponents, unusual questioning of motives, unusual tendency to magnify harm or disagreements and unusual emphasis on personal sovereignty. Even if challenging, vaccine distribution looks easier to achieve than other related virus challenges and may help to bring people together, to a more constructive degree. Doubt and questioning are great tools but, when trust is breached, it can become awfully difficult to get constructive and engaging discussions going.
-
Vaccine distribution is the next hurdle. -It's a challenge from a logistics point of view (how to get the product from A to B to C etc). -It's also a challenge in terms of 'strategy'. The demand will outstrip the supply for a while. So, questions raised about 'equity' (...), how to balance central 'message' with local 'adaptation' (...). An interesting input which lays out choices: https://vaccineallocation.ariadnelabs.net/
-
^No problem, my heart rate remained below 55 the whole time. BTW, i typically 'enjoy' arguing with you 'cause it makes me think. Arguing online has advantages but it's sometimes hard to get a "feel" for the other. Just a few more thoughts. The sentence that appears unclear is simply that you mentioned in late April that the vaccines did not exist even though it was pretty obvious that they did. :) Following the vaccine development here was truly fascinating and the typical "process" was dramatically changed. Instead of sequential parts with pauses, the process was massively transformed to perform several steps simultaneously and to lessen delays. Also, for instance, in order to reach targets or triggers for efficacy, lower numbers were used in order to make progress, assuming previously documented trends continued. It was a massive transformation simply unthinkable a year ago. Can the process be improved more? Likely. i guess if you're the moderator in the game, you want to move fast enough and not too much and of course, things always look easier in retrospect. From my perspective, it became clear that vaccines were slam-dunks only very recently. You may want to remember also that vaccines are coming out way earlier than usual vs longer term safety profile and there may be surprises along the way. And who will be blamed then?. i still see people from a clinical standpoint about a half-day a week and, anecdotally, even if my area is not really conspiracy-prone, many of the population at risk hesitate to take the vaccine or have decided to wait for more data to come in, given the new-normal. True even for those with high risk and their individual self-risk assessment needs to be respected (the "they" call this social acceptance and it can be a pain, especially if negatively reinforced). Thank you for the perspective and the impact could have been significant but i remain unconvinced and, under present circumstances (last few months), it would have been really difficult to compress the process more in order to get more 'uncertain' vaccines out earlier. But i'll keep an open mind, especially if contemporary evidence comes along. Anecdotal: Today, i'm preparing a report about a 'situation' where two 'experts' have reached diametrically opposed 'opinions' (that's usually when i come in). Typically in these 'cases', i come up with my own conclusion which may side with one side or the other. Interestingly, in this specific case, the opinion that is crystallizing is that both opinions are diametrically wrong. ??? Some people consider this last scenario to be a form a bipartisanship. It's not. BTW, personal criticism is fair game, if done fairly and for constructive purposes.
-
OK. That helps. However accusing that "they" voluntarily and knowingly withheld lifesaving treatments is a pretty severe accusation, perhaps requiring a stronger evidence-based case. BTW, i acknowledge that results have been very poor in my province. You may be interested to know though that i've been personally and professionally involved pre-Covid in describing the appalling status of care in elderly homes and trying to do something about it. It just seemed like such a contrarian proposition then and 2 weeks ago, i had to listen to someone who described how she had done a great job at preparing (organization-wise) for such an event (good thing my side was on mute). Also, when 100% active, fighting bureaucracy was a daily occurrence so the bias aspect (risk taking etc) described is understood. Concerning the obvious to vaccinate aspect in April in NYC (percent positive peaked at 71.17% on March 28th), it would be nice to share credible sources for this or is it more of a hunch? On April 24th, in the FFH 2020 thread you mentioned: "Their restaurant bet via Recipe is simply not financially viable given how restaurants will need to restructure until a COVID vaccine exists." You've come to and shared instructive insights in this thread so i assume that you mean that "they" had material information which was not shared and which would have had a major positive impact on healthcare burden. i don't have access to privileged information but have followed vaccine development quite closely. Please instruct me. On May 1st, i put that in The Day after Tomorrow thread: You did not comment on that, then in that thread but, concurrently, you put that in the CV thread: I'm surprised Trump hasn't released the vaccine already. You know he's smart enough to get it done. ;) I thought that he made the bleach announcement a couple of weeks ago? SJ i may be just too dumb but i still don't see what was so obvious then.