Cigarbutt
-
Posts
3,473 -
Joined
-
Last visited
-
Days Won
1
Content Type
Profiles
Forums
Events
Everything posted by Cigarbutt
-
Oh, it's even better than that. Here's a link to an interesting article in New York Mag which notes that we've had the vaccine available since last January, and we elected to not use it: https://nymag.com/intelligencer/2020/12/moderna-covid-19-vaccine-design.html So, what's interesting is that the outbreak in NYC showed a 19% Infection Fatality Rate for people 75 years and older during the outbreak last spring. Despite the fact that regulators knew very well that the IFR was ridiculous for that age group, there didn't seem to be much of an effort to seek volunteers from the highest risk groups to take an untested vaccine when regulators knew very well how lethal the virus was for them. In fact, they were operating under the assumption that ~60% of people would eventually catch it unless a vaccine were available, which tells me that they were completely comfortable with the notion of tossing under the bus 19% of 60% of people who were 75+ years of age. Fast forward to November 16, when the Moderna vaccine was announced, and they still don't seem to be in a big rush. On Nov 16, the US had a total of 11.5m cases and yesterday there were 15.4m. Cases have grown by nearly 4 million since the vaccine announcement. Plug in whatever population level IFR you think is correct -- maybe 0.4%? So, they've basically sat back and watched 16k additional Americans die since that announcement, and most of those will be concentrated in the oldest 10% or 15% of the population. They imposed a population wide risk preference on a sub-group that is at demonstrably higher risk. If they give it another week, maybe there will be another 1 million new cases and there will be another 4k deaths baked into the numbers. SJ Sure, unnecessary delays and institutional inefficiencies should be prevented, identified and improved upon. But why do 'we' have institutions like the FDA? Personal belief: The development of CV vaccines, overall, represents a great achievement and the result is some kind of a bipartisan (bipartisan in the sense of cost-effective collaboration and cooperation). Still, can 'we' do better? You bet. @SJ The assertion that a vaccine should have been used in March and April in the NYC area is interesting. Is it possible that this is a case of retrospective analysis gone too far? (Personal note: i'm still asked periodically to produce motivated opinions about things which happened in the past. A key aspect is that one has to try to travel in time in order to assess what a reasonable person would have done, under the circumstances and given the data set available, at the time. Starting the analysis thinking "they" are evil typically does not produce solid evidence). It's interesting to note that the "they" people (whoever they are) who act as intermediates between vaccine developers and the end users are also the same "they" people who are trying to define the distribution and allocation strategy for the vaccine. Why is that? From a pure free market perspective, the vaccine should go to (should have gone to?) the highest bidders. No? Or at least, from that same perspective, the vaccines should be offered to the potential (super-)spreaders first (irrespective of the disease potential which is low, overall, in this group) so that restrictions are lifted and the economy gets going. How would that go from a cost-benefit perspective? (i remember your previously documented thought process about individual cost-benefit assessment and the vaccine) Why will the allocation strategy be different? Of course, mistakes for allocation are being made at this point and in 8 to 9 months, 'we' can criticize the process. (personal bias revealed: i tend to respect people who work in the trenches)
-
Before moving to the 'curiosity' part, on a net basis and perhaps in addition to short term opportunities that may be spotted based on short term issues, the coronavirus impact will end up being positive for markets. You also have to assess the host but that's another story. On 1. Bed capacity is based on the physical beds (assumed to be available and functional (equipment and personnel)). There's always the possibility to work over 100% capacity, even in ICUs, simply by redesigning the space, redeploying available equipment and re-allocating human resources. Adaptive potential can be very significant. i remember specifically being involved a long time ago when a never ending string of ambulances were bringing women serially shot by somebody who thought he knew better. Capacity to adapt is one of the great qualities of humans. But this adaptation plays out on a daily basis, to various degrees. In my area, it's not unusual for emergency rooms to often function at around 120% of capacity for long and recurrent periods. This is more difficult to achieve acutely in ICUs and pressure build-up there will tend to cause major surgical procedures flow to be slowed down or stopped. The US is not used to that but it's not that unusual in Canada. An interesting aspect is that smaller hospitals in the US are seeing unusual activity levels due to Covid and, typically for these smaller operations, the 'capacity' is partly theoretical and when, in practice, the capacity is needed, they are meeting resistance along the supply chain, especially for specialized and dedicated personnel. Ordinarily, these smaller hospitals can transfer excess and unexpected surges in demand to neighboring hospitals but, these days, the capacity issues are widespread and people may have to be transferred far away, out of state etc. In some places, they built temporary 'field' hospitals but it's hard to ventilate somebody in the parking lot. On 2. This is a tough question. There may be some of a) and b) but it's mostly c). Last spring, there were some discussions between folks in my area and people on the ground in the NY area. This is not a discussion for this board perhaps but to help with perspective you may want to think of what you would do if in charge of a hospital near where a plane crashes. There would be a demand-supply mismatch and this is covered in training ie who to attend to and who to provide terminal assistance to. Those who work in war settings are also familiar with this. There are accepted triage criteria based on severity of injury, chance of survival etc. It's a situation you want to avoid but, if forced to, there are reasonable (but painful) ways to approach this. Specifically for Covid, i've seen protocols that were prepared, but not used on a large scale. The protocol 'works' for the majority of cases and for the debatable scenarios, there is usually a team of three or more people recognized by peers who can take the decisions. On 3. You may have heard that nurses from the mid-west went to the NY area at some point and there was some return in favors recently but this is not typically a cost-effective solution. If the help is coming from a different area, there are differences in equipment, protocols, rules and customs. The training and adaptation period likely negates most of the positive value that could be eventually obtained. In my area, there were attempts (mostly failed) at disparate resource re-allocation but it was discovered that brain surgeons are not that effective at elderly diaper changes. It would be interesting to read a diversity of opinions. i'm 90-95% retired but have some experience ranging from on-the-ground to decisional, and just finished a conference call. In my area, media will announce later on today that 50% of regular hospital activity will be curtailed across the board until further notice which means likely well into 2021..This too shall pass and all this is no big deal for investments but it is a true humanitarian crisis. At the end of the call, it was announced that the topic next Monday would be a review of end of life care decisions..
-
i guess that's the idea and it does get pretty dark sometimes. On top of what you describe, -It would be plausible for someone to go for the test in the AM and get a Ct of 22, in the PM the same day at 35 and the next day at 26. How can this be useful from an individual perspective, at this point? And this variability does not even include the basic fact that viral loads are dynamic in nature, it only includes the embedded statistical margins of error.. Taken at the population level, the statistical errors tend to cancel each other and may help more but the Ct-threshold value remains a qualitative input that needs contextual interpretation. -The quantitative aspect can be improved with context. If disease prevalence is high (ie virus % more than 5% in population tested), the false negatives are much less of an issue (this is a simple mathematical fact if you spend 4 minutes on this). Let's say you test for gonorrhea in an at-risk population with 'community' spread, the positive predictive value will be high (number of false positives will be low even with less than 100% specificity). However, if you test for the same disease in a low-risk population in an area where community spread is absent, the positive predictive value will be low, ie if you test positive, there will be a high chance that it is false. The false positive issue where coronavirus spread is wide is an irrelevant one. ----- The false positive rate is a reasonable concern and the issue arises because of uncertainty. It's too bad some quarters exploit the uncertainty to seed doubt theories. This is an investment board and the interesting aspects are the potential impact on investments and the analytical challenge. Last June, when this Ct-threshold issue was raised, the associated working assumptions (underpinnings of various doubt theories) were changing from the deaths will be counted on one hand to: it doesn't matter if hundreds of thousands die because they're dead-weight anyways and won't impact my portfolio, i would sell a family member for a profit if i could and to be involved in the market meant that you should be a socio-path. To better understand the spread phenomenon going on right now (not the virus spread) and to avoid clogging this site, i've exchanged elsewhere on the topic. Recently, someone blabbed out a post on the false positive doubt theory. During the exchange, it became clear that the person had shallow understanding and used tribal-type of analysis. The point of the person what that the CV story was fake news and the virus did not really exist. When confronted and cornered with counterfactual analysis, the person spontaneously switched to another theory and suggested that the virus landed in America in 2019 and had become widespread. When i suggested that it was hard to reconcile that the virus was nowhere and everywhere simultaneously, the person reverted to ad hominem attacks. ::)
-
For a long list of reasons, the Ct-threshold result is much more qualitative than quantitative. Countries which have been highly effective at containment could certainly wonder if they did too much to contain by, for example, wondering if using a lower Ct-threshold value would have resulted in the same level of containment with less restrictive measures. It is ironic that the same question is being asked where spread (contagious transmission) has been so rampant. In areas of high and persistent spread (high and rising positive rates), the additional value of more robust standardization of Ct-threshold value is like having the possibility to drive a Ferrari in dirt track racing.
-
What do you mean by false positive? -not contagious, no disease, no virus (true error) -not contagious, no disease, immaterial virus -not contagious, immaterial disease, virus+ As you likely know, the distribution of results along the Ct-threshold axis is different in the community vs when becoming hospitalized with Covid-19 confirmed by both clinical criteria and PCR test. Still, the trends in positive tests and test positivity in the community vs hospitalizations tend to be correlated. Do you think people who have become hospitalized with Covid-19 are falsely labeled positive as a result of the casedemic?
-
Two days ago, I participated in an online interactive review which is relevant for this military recruits study and its interpretation. The 60-minute review was health related and the word virus was not mentioned once which may be a sign that focus may have to go back to the host at some point. The review was a discussion about tools to assess studies and include in an evidence-based framework. The discussion was made necessary and relevant due to the fact that, for that specific field in question, in North America, there is an explosion of data, an incredibly high number of unnecessary procedures (waste) and an incredibly high number of poor outcomes (harm) and people are starting to notice (trust issue). One of the underlying messages was that one can ‘massage’ the data, the analysis and the interpretation (depending on incentives). But there are ways to help sort this out. This was relevant also to the analysis of various healthcare stocks I’m following as it seems to me a natural outcome of all this will mean, eventually, a very significant downsizing of sales and a shrinking market. It is also coming down on me that the polarized approach to the virus (great aspects, ie vaccine development and inefficient policy due to failure to coordinate and collaborate) closely parallels the growing issues for US healthcare overall (great aspects combined with a growing divide in the unusual hybrid approach) explaining the overall high costs and the overall low outcomes. More to come on that front for sure. There are two major problems with the interpretation of the military recruits study. First, extrapolating on the ‘intent’ of the study and second, the issue of generalization from a sample (unusual sample). 1st The questions (2) asked upon initiation of the study are: Under a standardized approach (and ideal in some ways), can spread be reduced to zero? and can asymptomatic transmission occur? These questions were reasonably answered and the answers were offered for peer review. Starting the process of retrospectively asking questions (and providing answers) after the study is complete is associated with very real and significant analytical risks. Asking questions is fine but providing answers then requires more work. That’s how blockbuster drugs for hair loss and erectile dysfunction were discovered. Companies did not start marketing a drug because they noticed unusual side effects while doing studies for a different question, they reframed the issue by asking a new question and by doing further studies and going through a systematic process. This example hides the fact that this exercise is a clear example of a survival bias as most unusual side effects and related hypothesis generation do not resist the test of time (analysis) after. To affirm that mitigation efforts for this virus “don’t work” because of this study, with some recruits coming in positive after a quarantine to start with, is a very weak assertion. 2nd The more the sample is different from a population, the more one has to be careful about generalization of specific findings. The military recruits’ situation was not a ‘lockdown’, it was a situation associated with some restrictions which, fundamentally, did not change their fundamental training. Basic tools such as safe distance, masks, self-quarantine when sick or exposed etc are not “lockdowns”. These tools are like the standard practice of giving oxygen to someone coming in with what looks like a heart attack. AFAIK, there is no definitive evidence showing that it ‘works’ but it’s done because it connects a lot of dots (easy, standard, low cost, makes sense scientifically and from a common sense point of view). If somebody doubts that, they can do or support doing studies to disprove that but that somebody should be careful before suggesting to stop oxygen use while the person is having a heart attack, especially if the motivation is that a mask is a threat to his or her freedom. In this thread, I’ve spent some time trying to disprove a fair amount of assertions of various levels of quality. So I’ll ask the following question: Fact: When including countries of a certain size (population large enough) and with a large enough GDP per capita, you end up with about 20 countries. In this group, since last May, by far, the US has reported the highest Covid-19 death per capita (even higher that the “high mortality” countries) and trends indicate that it will remain a clear leader for the foreseeable future. Question: Why is that? Is it because masks don’t work? The following answers will not be accepted: the virus was here in 2015, it’s China’s fault, it is what it is, we are turning the corner, Cuomo is dumb, so and so who is ugly had a hamburger yesterday, people don’t take enough zirconium, have no access to hydroxyfuckinqueen or to Bolivia’s health-minister-approved toxic bleach. My area is only a province and not a country but, if it were, it would take the #1 spot from the US for worst performer on the death per capita competition. Just a few days ago and a few kilometers (1 mile = 2.2km) from where we live, in a shopping center, there was a “demonstration” of a group (an anti-mask group) who “occupied” key walking space at the center of the shopping mall, dancing and singing unusual slogans. Why would you belong to an anti-mask group (waste of time)? Why would you participate in such a demonstration (waste of time, counter-intuitive and counter-productive)? Why would you put such a demonstration in the middle of an enclosed space at a time when it is most crowded during a period of rampant community spread in a “red zone” (dangerous on top of all the other reasons)? The most ironic part of all this was that there was this lady wearing a mask and doing her usual shopping who thought people had formed a group to show support for healthcare workers, so she entered the dance only to be told that she didn’t ‘belong’ and she was kicked out for fear of ideological contamination. Apologies for the length of the post and the ranty aspect but, yesterday, I ‘visited’ the huge tent beside my regional hospital and I still have (mental) nausea. Even if nobody reads this, writing it was therapeutic. It's not the ignorants that worry me.
-
i'm open to such views and even sympathetic to some aspects. For example, the 'costs' related to school closure (contributing to ignorance) are significant and i've pushed and rooted for maintenance and re-openings especially for younger cohorts. In my area, which is a typical example of collective individual massive failure, schools have contributed to the spread and there has been a 'price' to pay but it is true that younger children don't contribute to the spread in a major way and school 'cases' have been typically fed and nurtured from the community to the school and not the other way around. BTW 'isolation' of the vulnerable, frail and old is not a 'new' phenomenon with Covid. It's just that people talk more about it these days. If there's something that has become clear IMO, it's the fact that mortality and hospitalizations in a big way have occurred after rampant and persistent community spread and wishes to protect those at-risk have systemically failed to a large degree. In my area, January is typically a difficult month for healthcare in general, including hospitals and i just adjusted expectations taking into account evolving trends and January looks bad. i would offer the opinion that, for my area, there has been a massive failure of cost-effective collaboration and cooperation. This has been compensated partly (for the direct, indirect effects) by public entities going into debt but people, at large, again are wasting another crisis. i realize there is a critical mass and that critical mass is composed of ignorants (this is an interesting challenge) and of stupids (..). i was listening to a Sweden MD a few days ago and she explained that vaccine hesitancy and outright hostility is on the rise in Europe in correlation to how countries failed to control a relatively simple virus and she included her own country. People, in general, are losing confidence in a self-fulfilling way. Disinformation and misinformation are root causes. To show a degree of openness, here's a modified text from Mr. Bhattacharya: Lockdowns, of course, are not all that prevents the global economy from thriving now. People the world over have also changed their behaviour out of fear of the virus, with less trade and — therefore — less wealth spread. But mandatory lockdowns have costs. That they are not the only source of economic pain is not a reason to ignore their impact. Ending "lockdown" is the objective and the best way to achieve that is through sensible and cost effective collaboration and cooperation. The reason why my area is doing so poorly overall is not because of variable levels of 'lockdowns'. My regional hospital just set up a large tent outside and winter is coming.
-
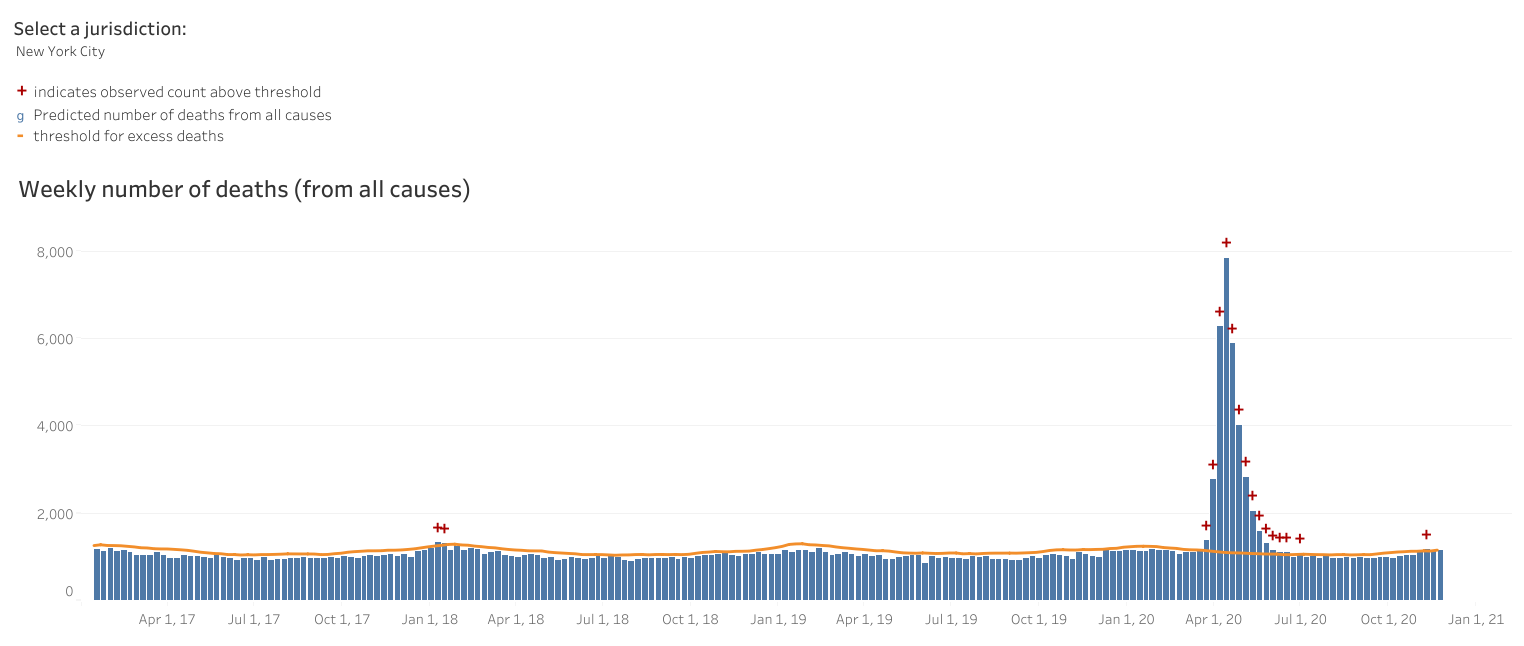
For those interested, below is a link to a recent study looking at years of life lost per Covid 'case' leaving in a body bag. TL;DR version: They evaluate with some adjustments (mostly guess) that the average years lost per case is about 13. Their work is exploratory but is also deeply flawed from an analytical point of view. i think their adjustment for co-morbidities is way too optimistic. They have to compare their Covid case group to the general population and they use the typical bias correction tools but, fundamentally, there are essential variables that cause certain people to get sick and die that are simply not captured by reported co-morbidities and related adjustments. There is a massive selection bias risk which suggests that the years lost per case is much less in reality, perhaps something around 50% less. That would happen to fit with local anecdotal experience. And is supported by the NYC inverse pent-up demand pattern that has not shown up so far, see attached. https://www.medrxiv.org/content/10.1101/2020.10.18.20214783v2.full.pdf From a pure investment or 'economic' point of view, these years lost are immaterial (unless comfortable with price action and other momentum strategies) and, in fact, from that perspective, reaching for maximum vulnerable mortality would likely add extra few points of return in the next few years. ----- The following is only if one's empathy reservoir is above zero. What is a life worth anyways (expressed per years lost or whatever)? There are several answers and sometimes one needs a number. In the 80s, in various developed places including the US, it was shown that increasing the speed limit on a highway resulted in economic benefits for some (reaching destination faster and more 'productive' output) while resulting also in an increased number of deaths (from vehicle accidents). While a speed limit has clear individual implications, there's also a collective thought process since humans have decided to band together for a while. The issue: the people gaining ($) from higher speed limits are not exactly the same losing (life, reported in $). So what to do? Whatever one does decide, one has to 'decide' what is the value of one's life, preferably another. Maybe that's a specific area where the one has to be tempered by the we. In the sense that 'we' can trust.

-
@petec You make an excellent point. From a different perspective, a solid run-off operation is worth a significant premium to book value and sophisticated players like Omers were ready to pay such premiums at end of 2019. Fair value at end of Q1 was not representative of true intrinsic value and the sub is being sold in Q4 (3 quarters seem like an eternity these days). :) It's not exactly the same but it feels a bit like (my perspective; i was mostly long then, parent, various subs etc) when OdysseyRe and Northbridge interests were offered to the public. The contract with Omers contained clauses to buyback the 40% interest within the next few years. It's a capital allocation decision and it can make sense (it may make even more sense with further corporate announcements) but the hurdle rate is relatively high. @SJ It feels like Omers is doing the right things, given its mandate with both upside and downside limited and embedded 'reasonable' returns. @Crip1 FFH has always displayed unusual creativity for liquidity management which has clear upside potential but comes with the associated risk that they may sometimes run low. Selling is always the hardest part.
-
Scratch that. See below. They're the same subs. Looks to me like Fairfax (60%) have made a nice gain on this sale ($750m vs a carrying value of $605m, with a possible $237m to come). This would imply OMERS (40%) got $500m plus $158m contingent, which means they may well have recorded a loss - unless of course they got better terms than FFH, which I suspect is likely. From the 3q interim: On March 31, 2020 the company contributed its wholly owned European run-off group ("European Run-off") to RiverStone (Barbados) Ltd. (“RiverStone Barbados”), a newly created joint venture entity, for cash proceeds of $599.5 and a 60.0% equity interest in RiverStone Barbados with a fair value of $605.0. OMERS, the pension plan for municipal employees in the province of Ontario, jointly manages RiverStone Barbados and had contemporaneously subscribed for a 40.0% equity interest for cash consideration of $599.5, based on the fair value of European Run-off at December 31, 2019 pursuant to the subscription agreement entered into on December 20, 2019. I am quite happy to see it go, frankly. I don't think the market gives runoff the credit it deserves and capitalising the cash flows up front to fund hard market growth in subs the market does understand is OK with me. i'm eager to learn but don't come to the same numbers. At end 2019, book value of the sub was 750.5m. Ultimately, with measurement adjustments after but based on yr-end, Omers paid 599.5m for a 40% interest, suggesting a 1.5b value for the unit without a control premium. This implies a 895m value for FFH which, i think, was written down to FV of 605m in correlation to negative results in Q1, including investment losses. i understand FFH will receive proceeds of 750+235.7=985.7m for their 60% deconsolidated equity interest so (assuming Omers gets the same terms) Omers should be getting 500+157.1=657.1m. One attractive aspect of FFH over the years (my humble perception) is (was?) that market recognition of value in the short term was not really relevant given a long term orientation. Even if felt to be obsolete, i have difficulty understanding why one should long for immediate market recognition when one of the principal lever of value creation would be share repurchases.
-
-Mixed feelings about the monetization of the European run-off business i had heavy exposure when run-off was formed in 2002 for the US run-off so there may be some unwarranted sentimental value but the run-off business they have built over time, including the European run-off, had reached crown-jewel value IMO, especially taking into account the possibility of huge opportunities in the future. Objectively, one has to look at what is gained on top of what is lost. They are getting a 'good' price and the cash inflow will be welcomed flexibility in this time of uncertainty and hard market. i guess it all depends on what they opportunistically do with the money. A disappointing aspect is that, if everything goes according to plan, 40% of the 15-20% premium they are getting now for the reincorporated unit will be going to the recently joined partner, Omers.
-
Yesterday, one of my daughters (the one who tends to ask questions i have no reasonable answer to) sat down for a chat. Summary of the conversation: -Why will we have to curtail activities with family and friends for the upcoming holiday season? -Because of those who don't know and those who don't want to know. Don't let it control your life, they say.
-
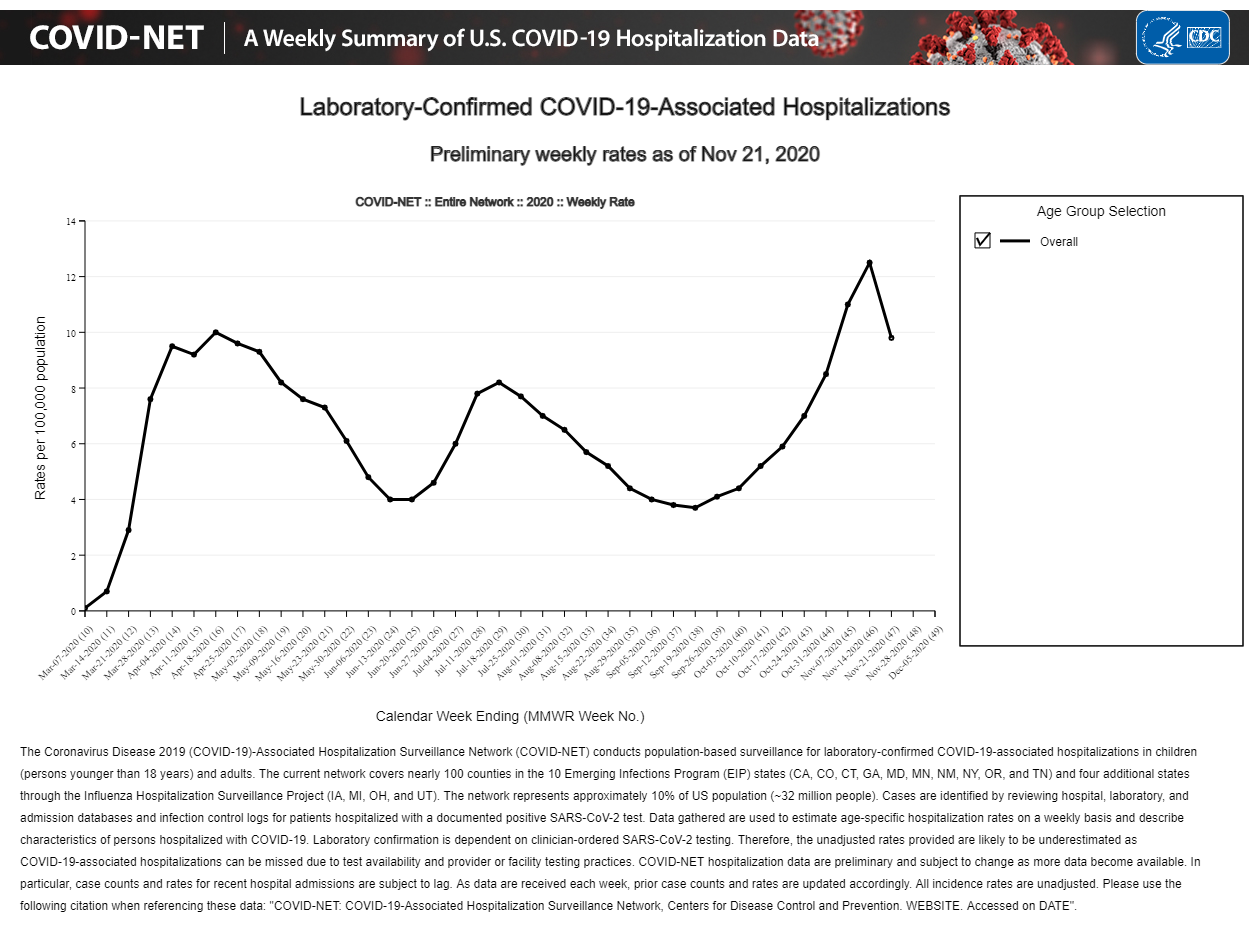
Investor20, i will engage here based on your question but have decided to avoid, to the extent possible, clogging this potentially great investment board with unnecessary and irrelevant posts. As you seem to know, my area has done VERY poorly handling the coronavirus episode but it’s not surprising given the chronic, well known (at least in certain circles) and deeply entrenched institutional weaknesses. However, I have been surprised by the extent of the underwhelming response in the US and I’ve spent time engaging in various online platforms dealing with the virus on America soil and i’m starting to understand better. The ivermectin comment was related specifically to Australia. See their NPS website for general recommendations and specific and evolving guidelines for ivermectin. When all is said and done about Covid-19, it will be realized that several aspects that have been applied shouldn’t have and several aspects that haven’t been applied should have. Ivermectin is interesting and a case could be built that institutions did not move fast enough for specific issues. The point for Australia is that, in their specific case, policy design and application rendered the use of ivermectin (or hydroxychloroquine, zinc, vitamin D, melatonin, famotidine, aspirin, herbs etc) essentially a non-material aspect. And now, vaccines are coming and Australia’s plan is also likely to score high on sustainability, given residual path to herd immunity. Your post assumes a certain level of allocation between the “costs” of the “lockdowns” and the economic costs directly related to the virus spread itself. You seem to assume that most costs are related to the “lockdowns” without really detailing the counterfactual used to analyze. You may be interested to know that institutions in Australia thought about this as the pandemic evolved. See pages 17-26 and 27-41 of the following document for the data, analysis and thought process. Australia is a nice example (there are others) showing that it is possible to collaborate and to cooperate in order to both minimize costs and minimize health outcomes without the need to rely on unproven treatments to save the day and without the irrational fear of permanent “control”. https://grattan.edu.au/wp-content/uploads/2020/09/Go-for-zero-how-Australia-can-get-to-zero-COVID-19-cases-Grattan-Report.pdf Anyways, at this point, in areas that used various forms of let-it-rip ‘strategies’ and various of other forms of race to reach herd immunity, with vaccines coming, ivermectin and related should continue to be looked into but are unlikely to represent significant breakthroughs. Soon, Covid-19 will be, going forward, basically a non-event and what will remain are memories of unnecessary excess mortality, an extra 9.7T debt in the US (government and corporates, as of last November 26th) and a global debt situation that looks like this: All this during an era when records are being broken, in stock markets but also in the length of lines at food banks, in developed countries and in the venerable USA. Did you read and analyze the recent study using 500 times the recommended daily amount of vitamin D in Covid patients? And I doubt ivermectin will make a difference but you can carry on. PS Did you see the latest data released by CDC vs hospitalizations?; soon they will be right in showing a promising downward trend but that may be old news. See attached.
-
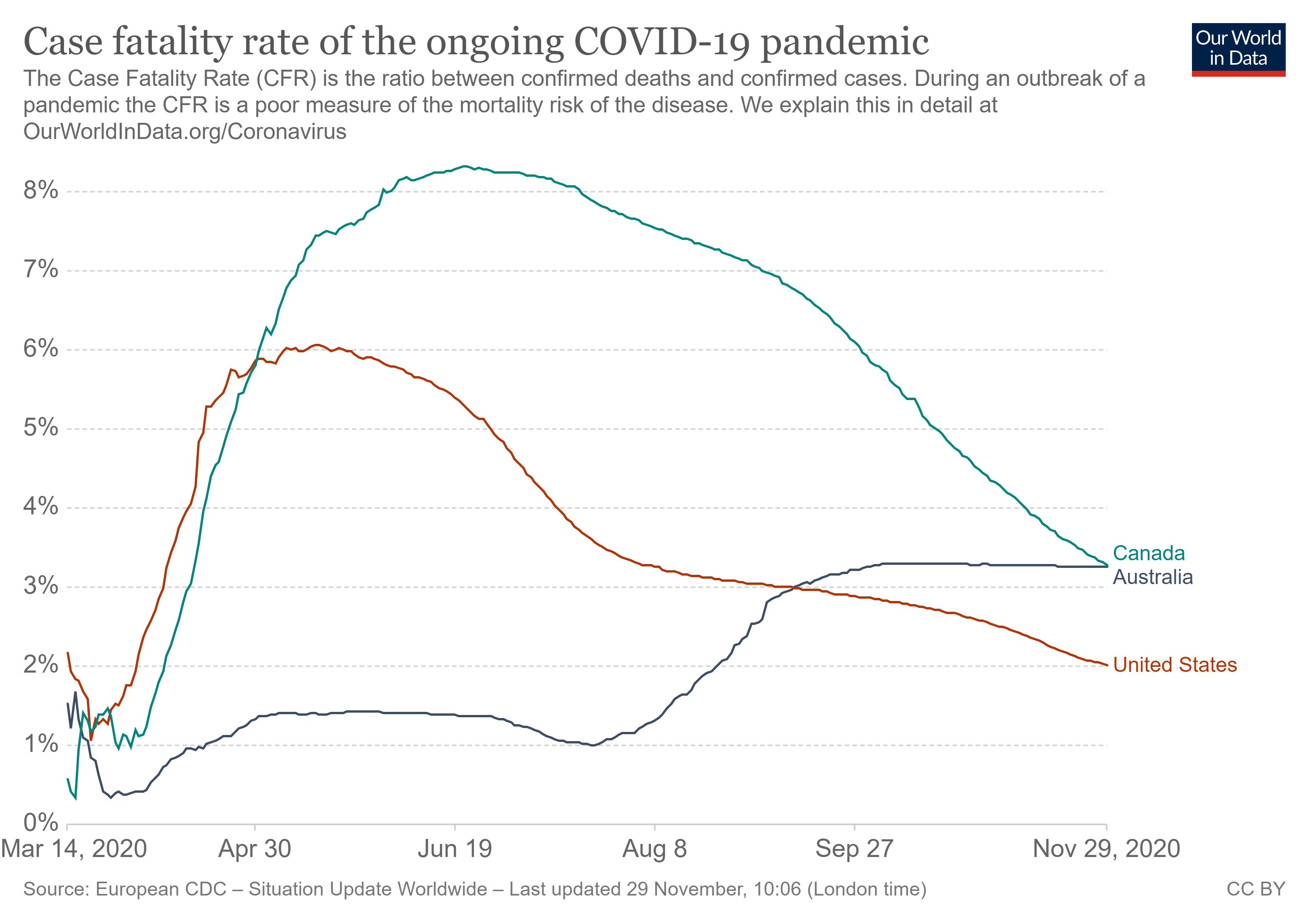
I'm not so sure that their lockdown is entirely responsible for their low case count. Australia is in summer right now and it's becoming increasingly clear that this virus is highly seasonal. We didn't hit zero in the US during summer. The numbers actually went UP as we entered summer coincident with lifting restrictions. This is interesting. Seasonal and other factors specific to the Australia region played a role, especially for the Victoria region later in the spread but, by far, evidence overall points to a very large and dominant positive response to effective policy. There is a lot to learn from Australia. Using the CFR as a tool (like any ratio used in financial statements analysis, it is important to analyze both the num. and the denom. to get to the underlying meaning) and comparing to the US (and Canada), on the surface and on a first-level basis, the declining CFR points to an improving survival picture (as claimed). Australia, on the other hand, shows a rising CFR trend. On a second-level basis though, when, last September, the Australia curve crossed the US one, it was a signal or a leading indicator in the direction of their stated goal: reaching zero case. The Canada curve is also shown. If one subtracts the results from my province, the curve remains the same shape as before but gets lower than the US for the entire period. The officials in my province sometimes suggest that 'we' have done relatively well but, at times, they have difficulty finding a region or country doing worse. Anyways, data is coming out for the Australia "flu" season and if it would be fair game to discuss the economic costs of measures that could be allocated to more than spontaneous and compliant reactions from citizens, but it looks like behavior modifications and restrictions had a massive effect (down) on seasonal flu numbers this year. Australia has produced very strong numbers overall (cases, percent positive rates, hospit., deaths etc) and ivermectin continues to receive proportional attention but, even if proven to be effective, alone or in combination, it would not have made a material difference in the aggregate. In his book Sapiens, Mr. Yuval Noah Harari, when explaining how humans came to dominate the earth, suggests that a main contributor to the course of events was the ability to cooperate in extremely flexible ways with countless numbers of strangers.
-
There is no embedded 'forecast' either for an individual looking for a specific property or real estate investments in general. It's looking at various scenarios and remembering that cycles can last a long time (both good and less good). It's fascinating to see that real estate values (including NYC, residential and commercial, as far as i can tell) have diverged from inflation trends for some time now and there are (may be) very good explanations for this. It seems to be though that (very) low interest rates are a key driving force and i wonder if that's good or bad or whatever. To paraphrase Mr. Grant, skyscrapers are the architectural expression of optimism, and no bookkeeper is likely to frustrate the way of progress.
-
Massive opportunity developing in gold stocks
Cigarbutt replied to Cardboard's topic in General Discussion
For the longest time, inflation, real estate and gold prices have had a tendency to correlate quite strongly. This has started to break down since the 1970s with real estate escaping upwards in spades (related to land prices mostly but who knows, even adjusting for houses getting larger) and with gold prices deviating strongly, up and down, but mostly up. See attached. Disclosure: i held (indirectly) gold bars from 2003 to 2008.
-
Make sense though. Large city with many renters, large population of young and single people and high cost. But I bet Seattle suburbs are white hot. I'm throwing 700k cash offers at 3bed/1bath 1,000 sq ft houses in the east bay of San Francisco. I'm not even competitive apparently... Suburbs have largely lacked the price appreciating that Appartement or houses in the city areas had. I lived in Long Island and now in Boston area and in both cases, houses were still below ~2005 prices. I think RE in thr city core might have doubled with8b the same time frame. If this trend reverses, it could have a long way to go, but I somehow doubt that it will. Actually good bay area suburban housing has been on fire since a couple of years after the GFC. The suburban city of Burlingame (17 miles south of San Francisco) has seen a 2.5X price rise for single family homes in the last 10 years (Dec-2010 to now). That is annualized appreciation of nearly 10%. If you take last 25 years for this suburb that number comes to about 7.5% annualized which is rivaling S&P returns (without dividends reinvested of-course). https://www.zillow.com/burlingame-ca/home-values/ For comparison San Francisco (SF) has appreciated "only" 2X in the last 10 years for single family homes (7.5% annualized) and about 4X in the last 25 years (for a return of 6% annualized). SF Zillow: https://www.zillow.com/san-francisco-ca/home-values/ SF Case Shiller: https://fred.stlouisfed.org/series/SFXRSA Thank you patience_and_focus, that was intersting (i like the SF area). i recently finished the traditional communication round to US acquaintances (most graduated in the late parts of the last century) who happen to form a relatively reasonable representation of the US territory. Covid was the big topic but, every year, it seems that the 'mood' tends to be related to trends in the stock market and, especially, real estate. i thought the following interactive tool was interesting (national, regional etc) https://www.visualcapitalist.com/20-years-of-home-price-changes-in-every-u-s-city/ -----)Back to the "Leaving New York City topic"; i like NYC too and the real estate market there went through Covid like a walk in Central Park but it seems to me anybody interested by NYC real estate in a big way should consider reading chapter 2 (pages 55-112 1996 edition) of The Trouble with Prosperity, written by Mr. James Grant. The chapter concludes with the 1995 40 Wall Street acquisition.
-
Practical follow-up Going for an additional test may increase the odds of a negative disease state, if negative but certainty is hard to achieve here. And then, if the test is positive, there's always the possibility that it's a false positive. Also, being free of disease today does not mean free of disease tomorrow. :) Statistical follow-up (just in case somebody is interested) Just like in any decision making process (health-related, investment etc), what you want are sensitive and specific 'tests' that help you keep or reject hypotheses (or investment targets). Disease Y N Y a b Test result N c d Where false negatives come is from the sensitivity aspect (a/a+c). Specificity is (d/d+b). That's the disease perspective. Another instructing aspect is the predictive value (test) perspective. Positive predictive value = a/a+b. Negative predictive value = d/d+c. So for a disease (or an investment) you want high sensitivity and high specificity tests for screening and high positive and negative predictive value on results to help delineate where the value is within the selected group. This may seem dry and irrelevant but it's quite useful (people do it all the time without realizing it) when, for instance, you meet people for the first time. You may ask them if they like sports to screen and then calibrate by asking if they enjoy rugby. By repeating the exact same test, you increase the odds for more precision but repeating the exact same test carries the same statistical limitations. ---- On the home oximetry. i've been following an interesting company that offers home services for people affected by chronic lung conditions. i think it is becoming increasingly overvalued (i may be wrong) and think that they wrongly focus on the equipment rather than the services side at this point although this may be related to how insurers deal with 'product' under present conditions. Anyways, they have the potential to provide, in real time, online monitoring of different parameters including oximetry in order to timely intervene and likely reduce complications, hospitalizations etc It's still unclear if the introduction of home oximetry would be cost effective on a large scale (for Covid-19 or otherwise) but, from an individual point of view, it's a reasonable option. There are smart watch options which are becoming interesting. Also, there are places where the idea is being tested. https://www.bmj.com/content/371/bmj.m4151 One characteristic of Covid (not unique but quite representative) has been the combination of a relatively comfortable person with unusually low oxygen saturation levels at the initial measure. These people were often clinical ticking bombs with very real and rapid deterioration shortly thereafter so the idea to detect a significant and relatively asymptomatic aspect is an interesting feature. The oxygen saturation to oxygen concentration (pressure) curve is interesting and offers valuable lessons for other disciplines. A very interesting feature happens when saturation reaches around and below 90%. This is related to a long evolutionary process meant to facilitate efficient oxygen unloading in peripheral tissues but has the side effect that the slope change around 90% can have sudden and disastrous consequences when it becomes systemic in the main circulation. i've seen this this play out many times (ages ago it seems) when making money around securities entering or leaving financial distress as the cost of capital has historically been quite volatile during these transitions. Of course, i've become increasingly confused as the changing slope concept has existed for centuries and has recently become irrelevant with firms entering financial distress no longer submitted to this natural law. In fact, in parallel to the Covid spread in 2020, firms entering financial distress often had access to lower cost of capital options!? i continue to wonder if historical easy money conditions have anything to do with this. It seems it's the same concept that Mr. Minsky used to elaborate his unstable stability concept. Anyways, home oximetry seems like a good and reliable idea if you're into self-monitoring. It is probably a better tool than home blood pressure monitoring. Home blood pressure devices are known to be quite imprecise. If you take it under standardized circumstances (ie once a day before breakfast), it may offer a reliable documentation of the underlying efficacy of non-pharma or pharma changes that are introduced. With blood pressure, there's the white coat syndrome aspect which basically means that your blood pressure may rise simply because you have reasons to believe that it should be, or needs to be, measured.
-
Short answer: The person may be right. Longer answer: This opinion shows the challenge when there are 'competing' schools of thought. When this issue becomes driven by 'us vs them', constructive discussions become difficult and often deviate from basic data, reasoning, weight of evidence etc. The opinion also shows the challenge related to balancing personal and collective responsibility. For various reasons, i've been involved in self-regulatory ventures which included to limit or terminate certain activities or even careers. A basic principle involved to respect alternative ways to think but the burden of proof should lie on the person voicing unusual or contrary opinions. So far, the evidence for the use of hydroxychloroquine at any stage of CV remains unconvincing and a lot of what the emerging school of thought is doing is to focus on the container, not the content. When assessing specific cases, the following type of comment sometimes appeared: [the] "doctor tells me they treated hundreds of patients and all of them are doing well". This was typically a massive red flag.
-
Given the description of the symptoms and 'epidemiological' circumstances, the two negative results are not enough to completely rule out CV. So, the idea is to behave as if the virus disease is present. Behaviors (altered or not) depend on various beliefs but information coming out of imperfect collective organizations whose recommendations are based at least on some level of trust and peer-reviewed processes suggests that at least self-quarantine versus others that are presumed to not have the disease is the minimal way to go. Further testing may not be helpful unless there is a specific reason. The above assumes a gradual process to recovery. If there is a specific reason to know or simply want to know, the way to go is to obtain another test in another testing area in order to control for collection technique, different lab, different test (antigen vs PCR) with a slightly different sensitivity/specificity (false negative, false positive) profile in general and evolving according to stage of clinical presentation. Another possibility is to wait for at least 2 to 3 weeks and get an antibody test.
-
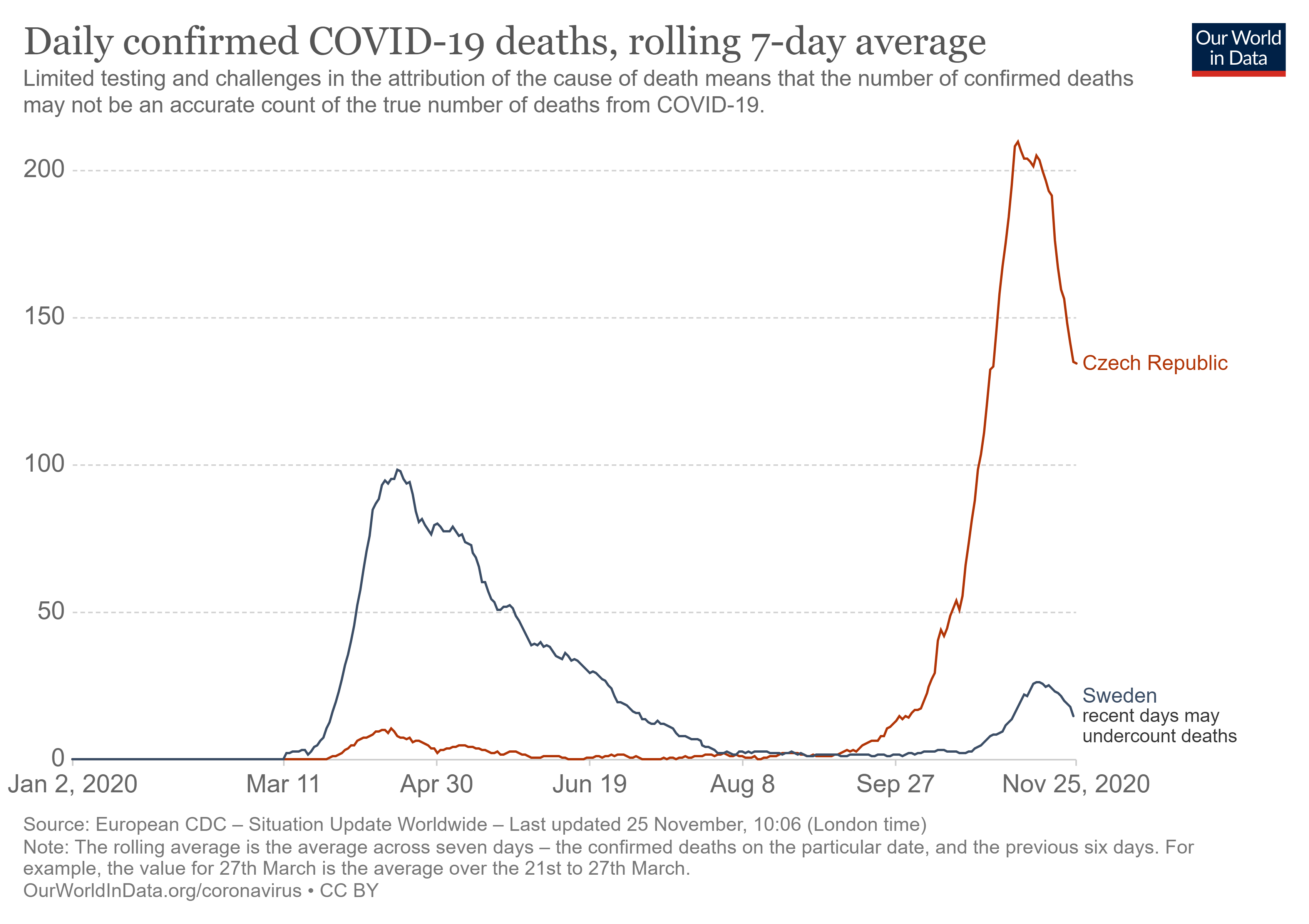
Thoughts on herd immunity This post is for analytical purposes and political aspects have been cured. The link to investments are: learning from mistakes and using a side-by-side-template approach described by Mr. Ben Graham to compare investments over time. My life is essentially a series of mistakes and subsequent studies of them and Mr. Graham's teaching is an example of an investment mantra based on survival from mistakes. It seems the US is reaching functional herd immunity with the present set of heterogenous restrictions in place. The Swedish case is interesting. They just released population antibody prevalence results with trends indicating that natural and 'pure' herd immunity is not in sight with antibody levels around one third. And they are, at this point, 'adjusting' restrictions. https://www.dn.se/sthlm/var-tredje-testad-stockholmare-har-antikroppar/ It has become fairly clear that their relatively different strategy has required a higher health-related cost for a very similar economic cost and they have recognized this to a large degree. They also adjusted along the way in order to improve. Even if the net outcome is relatively inferior, one aspect of their approach was sustainability. Compare to the Czech Republic. Sweden Czech population (M) 10.3 10.7 GDP per capita (k) 51.4 23.1 Covid-19 deaths (k per 100k) 65.6 75.0 European ranking* #7 #6 *ranking in the race for Covid-19 deaths per capita in EEA + UK Czech entered the race in good shape and (personal opinion) some of this was due to luck but it has entered a phase which will make it a clear winner. i would bet the GDP per capita differential will persist and perhaps even widen. See attached file for a visual. Some countries have followed a path to herd immunity at various levels of warp speed. For those who believe that a virus is a spreading disease with real consequences and who appreciate visual effects, the following is interesting: https://player.vimeo.com/video/466625351 Some people have started to retroactively look into this (ie the Sturgis motorcycle event, various rallies etc) and the potential conclusions are absolutely and relatively fascinating.
-
Frontline workers have proper PPE that protects them, and training. They are catching it from each other when their guard is down (in the breakroom, for example). This information is from my wife who is an HR manager at a large healthcare company (several hospitals and clinics with tens of thousands of employees). They are doing stupid things like having potlucks in the breakroom. This is interesting. Vaccine capacity vs demand mismatch will eventually be resolved but there will be a period over a few months that will require some kind of stratification introduced in the distribution logistics. Even if the protection aspect applies mostly, i would include, in the first line of distribution, frontline healthcare workers exposed in the following areas: emergency rooms, intensive care units, Covid-dedicated wards, nursing and chronic care homes, given that the virus spread is still rampant in many areas. Personnel retention in those areas has been a chronic problem and Covid-19 hasn't helped. This AM, i read (and find ironic) that the HHS is aiming for a top-down and uniform strategy for distribution, implying that states and individuals should have limited input in the process. In periods of vaccine scarcity, the idea is to optimize overall societal functioning. Given how things have evolved so far and given the polarization, this will be interesting to watch and this does not even include the aspect of vaccine nationalism.
-
Probability that covid will become endemic
Cigarbutt replied to LearningMachine's topic in General Discussion
Interesting but difficult to handicap. Who knows what will happen but it's likely that our future will mostly look like before with the exception of changes in relation to a relative acceleration of previous trends, with some areas more ripe than others. i would say business travel and higher education are good candidates. An interesting concept for the thought process is hysteresis (there are www opinions circulating now linking hysteresis with Covid-19). Hysteresis is used in many fields and i think it originated in pure physics but is also applied in 'softer' sciences, including finance. It has to do with an effect that persists after a temporary force or shock happens. Lingering effects of the virus will persist depending on the variables you mention but what will determine the outcomes is basically strongly tied to the condition of the host before. The hysteresis concept is also applicable for people who got sick (and getting sick) with Covid in relation to imaging changes seen in lung tissue. For Covid-19, it has been described (like just many cases of pneumonias) that patients who started to respond (mostly through their own intrinsic forces, supported by extrinsic measures) were showing deteriorating lung tissue anomalies on imaging, with a delay of a few days or even 2 to3 weeks before images started to improve, when the person actually felt fine and was often discharged. i think that's what Mr. Buffett said when he fundamentally discussed the risks related to waiting for a cheery consensus. -
:)
-
Probability that covid will become endemic
Cigarbutt replied to LearningMachine's topic in General Discussion
The following is submitted for analytical purposes and may have investment implications but political aspects have been sterilized, to the extent possible. FWIW, I think Covid-19 is likely to become endemic, within a year or two, but it will likely be an immaterial kind of endemicity. Below are the key factors considered as well as references used. -Availability of effective vaccines (% and strength of response, duration of protection) This looks promising but longer term duration is still unknown. How many in the population (at-risk and as potential spreaders) will take them is a limiting factor if vaccination rates don’t reach certain levels. Also, it’s still unclear if older and at-risk cohorts will be able to build and maintain sufficient immunity levels (available, on demand for antibodies or from “memory” cells). The typical FDA agreement includes to complete follow-up studies for safety and efficacy for at least two years. -Virus characteristics Many respiratory viruses are endemic, including the four well known common cold (beta family) coronaviruses. Longer term studies point to a very real risk of endemicity. More virulent CVs (SARS and MERS) seem to be associated with longer and more robust immunity. Covid-19 is kind of hybrid so common sense would indicate that endemicity risk is real. CVs tend to mutate less than influenza for instance (because of a very unusual and fascinating proof-reading mechanism during replication and specific to this class of RNA viruses) but this is both good and bad. The good part indicates that covid-19 will tend to be slow to genetically escape existing immunity but the bad part indicates that when a new genomic form with new characteristics is reached, this stable form may bear less favorable characteristics for the host (including for immunity) and may persist longer. Whatever residual immunity (natural or vaccine-related), reinfections are likely to be less severe which opens the eventual possibility of eradication to the same degree that it opens the door to low grade endemicity. -Population and environmental characteristics With the virus impact becoming less significant and with less public awareness or media attention, non-pharmacological measures will tend to be abandoned, not enough to cause major and widespread outbreaks over time but enough to allow endemicity in many populations. The virus has become truly global and the world has grown smaller. Seasonal and various environmental factors (for most areas of the world) may become a feature for Covid-19, following what other common cold coronaviruses have become over time. ----- So, on a weighted basis, it’s likely that Covid-19 reservoirs will persist over time but are unlikely to trigger material events on a global basis. For references, I was lucky to be able to listen to a very strong presentation 8 days ago by various ‘experts’. One of the presentations dealt specifically with immunity, reinfection risks and vaccinations. She covered, in a few minutes, most of the relevant research, some of which is mentioned in the CDC link found below (pages 12-22 for post infection immunity, pages 23-32 for reinfection risk). The study mentioned on page 28 is somewhat interesting (design, implications, despite limitations). Also found below is a link to a site monitoring progress on the vaccine front. The amount of human capital involved is mind boggling. The people involved have obvious financial incentives but there is an unusual amount of drive, especially in smaller operations. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2020-10/COVID-Wallace.pdf https://covid19.trackvaccines.org/vaccines/