Investor20
-
Posts
518 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Everything posted by Investor20
-
The anti-Trumpers wont agree, but if you follow the Great Barrington Declaration Herd Immunity is not a strategy, but inevitable. Herd Immunity, Dr. Bhattacharya says is like gravity. The plane is going to come down sometime. The question is how to land safely. This makes the therapeutics and vaccines much more important and only US government with Warp Speed project got them developed very fast. The shortest vaccine development I believe is for mumps with four years. https://edition.cnn.com/2020/03/31/us/coronavirus-vaccine-timetable-concerns-experts-invs/index.html The timetable for a coronavirus vaccine is 18 months. Experts say that's risky (April 1st) White House started working on warp speed project with aggressive timelines, and seems to be beating the 18 month time line which it self experts were skeptical. To quote from article "Dr. Emily Erbelding, an infectious disease expert at NIAID -- which is part of the National Institutes of Health -- said the typical vaccine takes between eight and 10 years to develop. " I'd say warp speed vaccine is something that makes me unwary if that means steps are being skipped. China and Russia are already bragging that they are ahead of the vaccine race. I suspect part of their lead is skipping steps. But what if skipping a step brings death to 0.1% of the population? That's 1.5M death... I'll trust to get a vaccine if all the steps of the stages have been properly respected. Anything else is just rolling dice. Apparently, the FDA is holding their stand toward pressure. Let's hope it stays that way. Trump has little to do with how fast a vaccine gets released... provided he does not force to skip steps. Tests take time and you can't make a baby in one month by making 9 women pregnant. You can however provide funding and make sure the production capacity is ready when it gets approved. But again, any government can calculate the risk/reward over 4T$ deficit VS 10B$ wasted production capacity. I'm sure even Canada, say's to it's pharmaceutical industries, money is no object. BeerBaron I am not sure if 0.1% (1 in 1000) death rate could be missed with a trial with over 30,000, upto 44000 in phase 3 - even at 1:1 treatment:placebo, that is 15000-22000 who got the vaccine. That would make missing at 0.1% 15 to 22 deaths. And would everyone get it or only older and vulnerable? Anyway 0.1% of 200 million would be 0.2 million. "The companies said in a press release that they would increase the size of the study to 44,000 participants, up from an initial recruitment goal of 30,000 individuals" https://www.statnews.com/2020/09/12/pfizer-and-biontech-announce-plan-to-expand-covid-19-vaccine-trial/ https://www.kare11.com/article/news/health/coronavirus/30000-volunteers-enroll-in-pfizers-covid-19-vaccine-trial/507-a6bfa39a-0822-4575-9667-5a15545667ca Pfizer COVID-19 vaccine trial reaches initial goal of 30,000 volunteers an additional 14,000 volunteers to expand the diversity of its phase 3 trial for a coronavirus vaccine.
-
The anti-Trumpers wont agree, but if you follow the Great Barrington Declaration Herd Immunity is not a strategy, but inevitable. Herd Immunity, Dr. Bhattacharya says is like gravity. The plane is going to come down sometime. The question is how to land safely. This makes the therapeutics and vaccines much more important and only US government with Warp Speed project got them developed very fast. The shortest vaccine development I believe is for mumps with four years. https://edition.cnn.com/2020/03/31/us/coronavirus-vaccine-timetable-concerns-experts-invs/index.html The timetable for a coronavirus vaccine is 18 months. Experts say that's risky (April 1st) White House started working on warp speed project with aggressive timelines, and seems to be beating the 18 month time line which it self experts were skeptical. To quote from article "Dr. Emily Erbelding, an infectious disease expert at NIAID -- which is part of the National Institutes of Health -- said the typical vaccine takes between eight and 10 years to develop. "
-
https://www.who.int/influenza/publications/public_health_measures/publication/en/ G L O B A L I N F L U E N Z A P R O G R A M M E Non-pharmaceuticalpublic health measures for mitigating the risk and impact of epidemic and pandemic influenza You have to download the PDF document. Quoting from this document: (NPI: Non pharmaceutical intervention) Page 2: "There have been a number of high-quality randomized controlled trials (RCTs) demonstrating that personal protective measures such as hand hygiene and face masks have, at best, a small effect on influenza transmission, although higher compliance in a severe pandemic might improve effectiveness." ........ Page 26 OVERALL RESULT OF EVIDENCE ON FACE MASKS: Ten RCTs were included in the meta-analysis, and there was no evidence that face masks are effective in reducing transmission of laboratory-confirmed influenza.
-
CDC Director Dr. Redfield said "I might even go so far as to say that this face mask is more guaranteed to protect me against Covid than when I take a Covid vaccine, because the immunogenicity may be 70 percent. And if I don’t get an immune response, the vaccine is not going to protect me. This face mask will. "
-
I looked. And there is almost no criticism of Trump in Feb/March. He is the President of the United States. He's going to get criticism (even if he did everything right). But blatant Trump-bashing was exceptionally rare on this thread. My guess is that you are recalling conversations from other threads. No need to bash Trump, the man is fully capable of speaking for himself this subject: “Just the other day, they came out with a statement that 85% of the people that wear masks catch it” “A lot of people say masks are not good, I’ll tell you who those people are, waiters.” "If we stop testing right now, we'd have very few cases, if any' https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/mm6936a5-H.pdf Please check page 1261 - table at top of page for "Reported use of cloth face covering or mask 14 days before illness onset" Mask use for Covid Positive group: Often: 14.4%; Always 70.6% (Total of Often + Always use of mask 85%) Mask use for control (negative) group: Often: 14.5%; Always 74.2% (Total of Often + Always use of mask 88.7%)
-
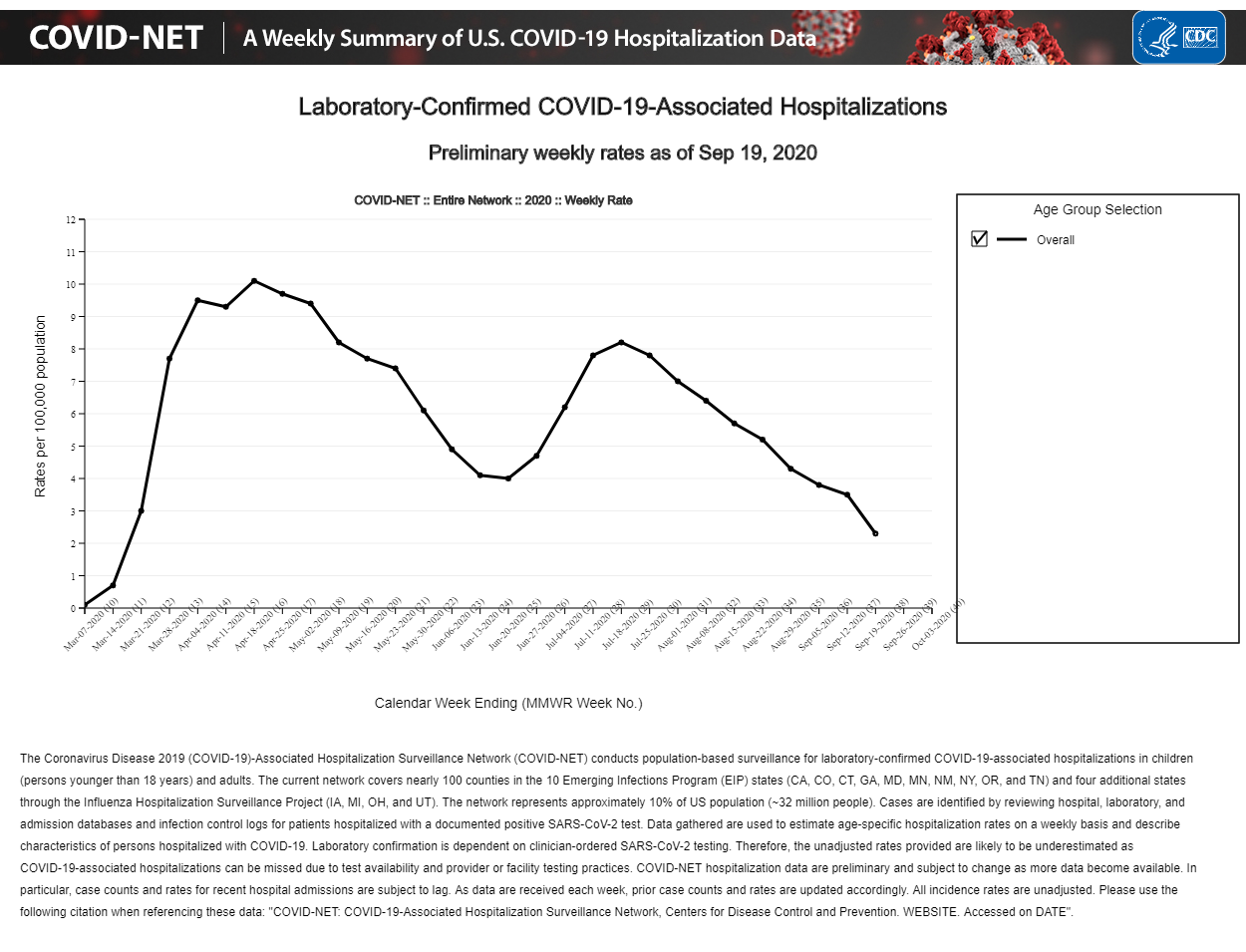
CDC is showing drop in new hospitalizations as of October 3, especially the 65+ years which is most important group from vulnerability POV. Percent hospital & emergency visits for both Covid like (CLI) & Influenza like (ILI) are down to baseline This is a summary of Positivity rate, new hospitalizations, Hospital visits...all down
-
Finally randomised clinical trial of Ivermectin+ vs placebo https://clinicaltrials.gov/ct2/show/results/NCT04523831 Of 556 patients who screened and were assessed for eligibility, 400 underwent randomization. Total 200 patients received active drug and 200 patient received placebo. Masking: Double (Participant, Investigator); Details of results including time to recover, severity of symptoms, side effects & all cause mortality are given in the link. This website is lot more readable on PC than on mobile phone.
-
Unfortunately CDC or WHO do not agree with this airborne transmission leading to clusters. After several changes in their guidances as described in below article https://www.indystar.com/story/news/health/2020/10/05/covid-cdc-updates-guidelines-include-airborne-transmission/3627932001/ CDC updates guidelines (again) to note risk of airborne transmission, says coronavirus can infect people more than 6 feet away The present scientific brief of CDC says "The epidemiology of SARS-CoV-2 indicates that most infections are spread through close contact, not airborne transmission" https://www.cdc.gov/coronavirus/2019-ncov/more/scientific-brief-sars-cov-2.html That is their guidelines are still focused on larger droplets and physical touch both dont lead to one person infecting many at a time, unlike airborne transmission one person can infect dozens at a time. It is really puzzling after many super spreader events indoors such as Patent 31 in church described in the Atlantic article, why they still think on these lines.
-
Hmm. It's almost like the "immunity" in herd immunity means something... Exactly. Which is why the herd immunity term in the general lexicon has become a complete misnomer. This virus will be around long after a vaccine is widely available but at some point (and a lot sooner than many think), it will no longer be an epidemic. Instead, it will become endemic in the population just like all the other respiratory viruses that circulate regularly. This is how previous pandemics ended - viral infections were never eliminated. Exactly Frank. Infact as per CDC, the emergency visits for Covid like symptoms (CLI) to hospital are already at about February level (my earlier post). The hospitalizations are about at middle of March. Yes we can count Covid positives. But ultimately its the hospitalizations that matter.
-
Emergency Department Visits Percentage of Visits for COVID-19-Like Illness (CLI) https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/10022020/covid-like-illness.html Week Percent of Emergency Room Visit 202039 (Sep) 1.9 202006 (Feb) 2.2 US is already below February in percent Emergency room visits for Covid 19 like illness
-
Agree there is clear waning of antibodies in not only NYC data but observed many places elsewhere. I am reading the 20% present new york antibody as simply last several months of infections, not cumulative infections from February. My understanding of T Cell immunity is it does not stop infection but reduces severity of infection. With this regard vaccines might not prevent re-infection, but only severity of infection: “if everyone gets vaccinated and we continue to implement the public-health measures that I have been talking about incessantly over the last several months,” Fauci said according to below article https://www.self.com/story/fauci-masks-after-vaccine
-
Not sure why you have such a hard time with stats. The data for 4/11 is a tiny sample and is an obvious outlier. The question is why? Sample size of 1131 is not that small. Its typically used for national polls. https://www.scientificamerican.com/article/howcan-a-poll-of-only-100/ How can a poll of only 1,004 Americans represent 260 million people with only a 3 percent margin of error?
-
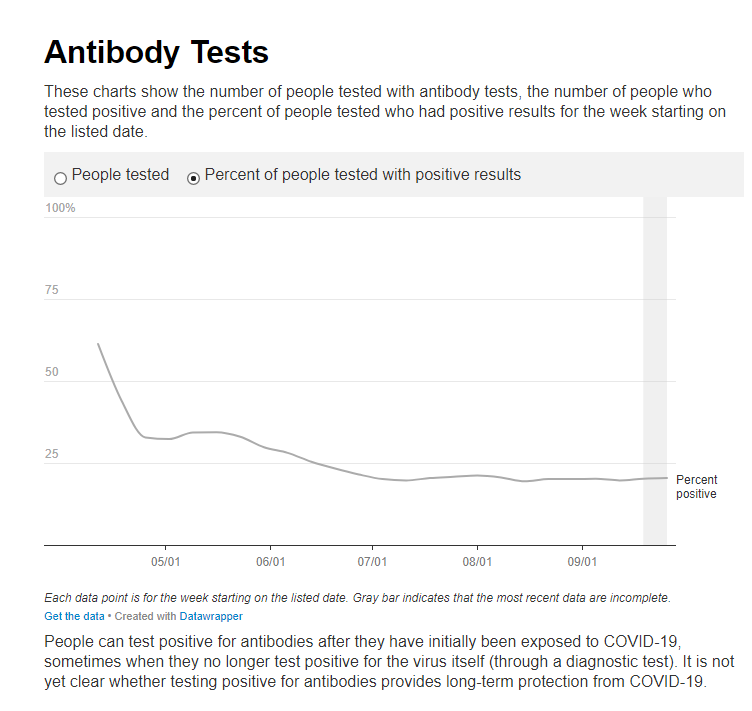
The NYC website is reporting 61.3% seroprevalence for NYC as of 4/11/2020, not for a borough or an area. Cigabutt, are you saying NYC is reporting wrong numbers? https://gothamist.com/news/nyc-map-coronavirus-antibody-testing-data-date NYC Releases Largest And Most Detailed Coronavirus Antibody Testing Data To Date, Aug 20, 2020 "At one point, the positivity rate of antibody testing soared to as high as 61% in early April. It has since leveled off to around 20% over the last three weeks." A lot of people seem to loose antibodies in very short time. The 61% on April 11th went to 34% on May 9th. Thats very concerning from vaccine point of view.
-
Its not cumulative. For cumulative the numbers will increase with time. The seroprevalence as per NYC website went down from 61.3% in April to 20% in September. That indicates people loosing antibodies, which I have posted before as a problem at looking at seroprevalence to check how many got infected. If you do cumulative it will be 61.3% by April plus however many infected after April. The numbers in the data base are given as fractions 0.613, is 61.3%. Look at the plot on the website. I also attached a screenshot of the plot with this message.

-
https://www1.nyc.gov/site/doh/covid/covid-19-data-testing.page New York City Percent positive for antibodies You can scroll down in above page to "Antibody Tests" click on percent of people tested positive. I couldn't get the image here, so downloaded the data associated with that plot using "get data" and given in below table. It started in April with 0.613, that is 61.3% seroprevalence in NYC! And ofcourse people got infected afterwards and there are reports of antibodies lasting only for 2 months, at least in part of the population. That is total infected in NYC is more than 61.3%. Am I wrong? Why so many report it is 20% infected in NYC? weekdate Percent positive 4/11/2020 0.613 4/18/2020 0.439 4/25/2020 0.328 5/2/2020 0.323 5/9/2020 0.343 5/16/2020 0.344 5/23/2020 0.33 5/30/2020 0.298 6/6/2020 0.281 6/13/2020 0.254 6/20/2020 0.233 6/27/2020 0.215 7/4/2020 0.201 7/11/2020 0.197 7/18/2020 0.204 7/25/2020 0.208 8/1/2020 0.212 8/8/2020 0.206 8/15/2020 0.194 8/22/2020 0.201 8/29/2020 0.201 9/5/2020 0.202 9/12/2020 0.197 9/19/2020 0.202 9/26/2020 0.204
-
Why is it that herd immunity would be the only factor? The household transmission rates are interesting. If herd immunity is the factor, how do you explain the following: -These and similar studies show that transmission rates for COVID in the household are way higher than for MERS or SARS, does that mean that herd immunity had been reached for those previous viral episodes? -Proximity seems to play a role (spouses vs others etc), so why not consider increased in-house basic precautions and basic distancing as relevant and important co-factors? -The study mentioned that self-quarantine (behavior) made a huge difference in transmission outcomes, irrespective of any theoretical herd, natural or innate immunity, so how does that fit in the mono-factor immunity theory? -Many places in the world have reached antibody levels higher than 30, 40, 50 or even 60%. If cell-mediated immunity is such a critical variable, why doesn't it prevent antibody levels from reaching such high levels? Look at the following. The study has significant weaknesses but it was made in a relatively controlled environment where herd immunity took a while to kick in: https://www.medrxiv.org/content/10.1101/2020.09.16.20194787v1 Personal note: my area recorded one of the highest prevalence of disease last spring. And now the same area shows a significant rise in cases, although, for a variety of reasons and including also a partial level (IMO) of herd immunity, this "second" wave should result in less morbidity and mortality. But despite this higher herd immunity obtained due to previous institutional weakness and basic competence issues, it seems that my area will do worse (because of persistent and widespread community spread) than most parts of Canada who, it seems, made a conscious step to not bet on the herd. " The seroprevalence fell in July and August due to antibody waning. " states the article you posted. The problem with seroprevalence studies are that antibodies are lasting only few months as seen in above study. Bill Gates said, we probably will need two doses of vaccines and quoting Bill Gates regarding side effects "“some of that is not dramatic where it’s just super painful". Now if only antibodies confer immunity and antibodies after vaccination last only few months, we are in trouble right? I always thought the vaccine development is also based on non-antibody immunity, but that applies to prior infected too. The article you posted makes that clear. The number of infected and immunity is much more than the antibody study results. We also see repeatedly cases fall once the seroprevalence reaches 20-30%. Sweden had 14% antibodies in July. Yet we dont see any second wave in Sweden. To take the seroprevalance of 14%in July and say Sweden has long way to go when we can also see the peak deaths in Sweden is in April! We can agree July is after April? https://www.thelocal.se/20200723/14-of-antibody-tests-positive-in-sweden 14% of coronavirus antibody tests positive in Sweden in July https://www.worldometers.info/coronavirus/country/sweden/ The other corroborating evidence is the one I posted before, spouse secondary attack rate below 50%.
-
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa450/5821281 The secondary attack rate to contacts who were spouses of index cases was 27.8% compared with 17.3% for other adult members in the households. https://ncrc.jhsph.edu/research/household-transmission-of-sars-cov-2-a-systematic-review-and-meta-analysis-of-secondary-attack-rate/ It also estimated 32.5% (95% CI: 7.4 – 57.5%) of households with an index case had a secondary case. Spouses had statistically significant (P<0.001) increased secondary transmission (43.3% of spouses were infected) compared to other relatives of the index case (18.3%), and adult contacts had significant (P<0.001) increased transmission (31.0%) compared to children (15.7%). Repeated studies have shown spouses of index case are infected less than 50%. In two confirmed cases I know personally, in both families the spouse turned out to be negative. In fact other family members got infected but not the spouse. The explanation that is given for less than 50% of spouses of index case getting infected is that about 50% have built in immunity even before covid infection. You have to add the Covid antibody for seroprevalence studies to this to get the percent immune to Covid. If you look at Florida, Texas, India. All of them have turned around (India just starting) and in the seroprevalence studies in none of the places is it above 30%. All of that is interesting, but none is particularly pertinent. The study that Spekulatius quoted was conducted during July, but the authors could not specify a particular collection of dates. In the absence of that, you need to assume that the data reflect mid-month, or July 16. So, the study showed that on about July 16, 8.3% of 328 million people had antibodies, or about 27.2m people, IFF you believe that dialysis patients reasonably represent the general population (more on that later). So if the sample were representative to the population, the study would suggest that 27m Americans had antibodies on July 16. On July 16, there were 3.7m officially diagnosed cases of covid. So, if the dialysis patients are representative of the general population, the true number of cases in the US would be 7.4:1 of the official number. So, where are we today? The US is now up to 7.3m official cases. If you believe the 7.4x ratio that Spekulatius' study would suggest, that would suggest that ~54m people would have antibodies today. So, that's a shade higher than 16% and herd immunity might be about 60%? According to this particular study, that's the math. Now, turning to representativeness of the dialysis group, we need to reflect on Spelulatius' assumption that these folks are representative. Spek would suggest that the presence of visible minorities would make the group representative. The countervailing behavioural assumption might be that any rational person with a comorbidity (dialysis requirement) would have been making extraordinary efforts to reduce their social circle to avoid covid. What is more, one must also question the extent to which dialysis patients are employed, because workplaces are an important place of exposure. If you are so sick that you require dialysis, are you sufficiently healthy to work. I therefore question the representativeness. The study is nonetheless valuable. But, perhaps in your own mind you need to multiply the results by some sort of scalar to reflect the potential for lower contacts among the dialysis group. So take the 16% antibody rate and gross it up as you see fit. The "finish line" might be about 60%. What is interesting about this study is that, if you believe that dialysis patients made a modicum of effort to reduce their personal contacts, a 10:1 ratio of antibodies to official cases might be supported by this study. Unfortunately we won't know the truth of the situation for another couple of years. SJ To the question how many are still vulnerable, it is relevant how many are vulnerable with zero antibodies. The most pertinent is that the weekly hospitalizations have dropped by 75% (8.2 on July 18 to 2.3 on Sep 19th per 100,000). That is US in hospitalizations is about same in first week of March! I still could not figure out how to include the image inside the post, but I attached the image. https://gis.cdc.gov/grasp/COVIDNet/COVID19_3.html
-
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa450/5821281 The secondary attack rate to contacts who were spouses of index cases was 27.8% compared with 17.3% for other adult members in the households. https://ncrc.jhsph.edu/research/household-transmission-of-sars-cov-2-a-systematic-review-and-meta-analysis-of-secondary-attack-rate/ It also estimated 32.5% (95% CI: 7.4 – 57.5%) of households with an index case had a secondary case. Spouses had statistically significant (P<0.001) increased secondary transmission (43.3% of spouses were infected) compared to other relatives of the index case (18.3%), and adult contacts had significant (P<0.001) increased transmission (31.0%) compared to children (15.7%). Repeated studies have shown spouses of index case are infected less than 50%. In two confirmed cases I know personally, in both families the spouse turned out to be negative. In fact other family members got infected but not the spouse. The explanation that is given for less than 50% of spouses of index case getting infected is that about 50% have built in immunity even before covid infection. You have to add the Covid antibody for seroprevalence studies to this to get the percent immune to Covid. If you look at Florida, Texas, India. All of them have turned around (India just starting) and in the seroprevalence studies in none of the places is it above 30%.
-
Hmmm... :) So, more absurd diversion based on the fact that the 'scientist' used essentially unsubstantiated claims, went through a non-peer-reviewed process and published the study in a non-scientific journal funded by a party who is closely aligned with somebody voicing unusual opinions and who recently got arrested for fraud: https://www.dailymail.co.uk/news/article-8738733/Study-claiming-covid-Chinese-lab-published-groups-founded-Steve-Bannon.html i think the word absurd applies but not in relation to the diversion you describe. Are you (like your Scientist-in-Chief yesterday) also confusing herd immunity with herd mentality? ----- In related news, Google just announced a deal with Singapore (i have mixed feelings about the Singapore model and about this deal but it's interesting) whereby good behaviors including vaccinations will be rewarded using some kind of nudge strategy, extending a strategy that was used during the pandemic in order to contain spread: https://www.bloomberg.com/news/articles/2020-09-16/singapore-to-pay-citizens-for-keeping-healthy-with-apple-watch This virologist does seem to have relevant background. She published both in animal transmission of viruses and coronaviruses. So whether Covid-19 came from bats to humans or not, she does seem to have expertise in that area. Pathogenesis and transmission of SARS-CoV-2 in golden hamsters By Prathanporn Kaewpreedee, Malik Peiris, Hui-ling Yen, Li-Meng Yan nature.com Viral dynamics in mild and severe cases of COVID-19 By Yang Liu, Li-Meng Yan, LKS Faculty, Tian-Xin Xiang thelancet.com https://muckrack.com/li-meng-yan/articles
-
Maybe you're pulling my leg but just in case you're serious. First, a picture is worth a thousand words but i owe you an (scientific) explanation for the partisan picture: Taking into account the pathophysiology of the virus, its mode of transmission and multiplication as well as socio-sanitary data from the area where the rally occurred, it's likely that many will become sick, some will be hospitalized +/- requiring ventilatory support and a few may have signed their own death warrant. For the method to insert an image (please accompany with a scientific explanation, especially for the causation part), you can use (click on) the bottom-left item on your screen above the smiling emoji and obtain: [ img ] [ /img ], then insert your url link with a proper image format so that it becomes: [ img ] http://www.blablabla.png [ /img ]. i also learned earlier this year (from an exchange between posters of whom at least two are vit.D fans) how to change the size of the picture to improve the 'fit'. For example: http://tylervigen.com/correlation_project/correlation_images/per-capita-consumption-of-cheese-us_number-of-people-who-died-by-becoming-tangled-in-their-bedsheets.png http://tylervigen.com/correlation_project/correlation_images/per-capita-consumption-of-cheese-us_number-of-people-who-died-by-becoming-tangled-in-their-bedsheets.png So, by using: [ img ] [ /img ] and changing it to: [ img width=# ] [ /img ], # being something like 200 to 900, you can adjust size. BTW, the correlation coefficient for the above data is a solid 0.95 so i've petitioned my local jurisdiction to limit cheese consumption even if it may have an adverse effect on vit. D levels at the population level. In a show of good faith, i will accept a recommendation to take vit.D during the next winter if you submit a specific product (i need help). Please not the product that contains fermented and rancid cod oil. Hope this helps but i'm starting to wonder. No, I am not pulling any body leg. I wanted to post a graph from a pdf article, not from a website. I can extract the plot itself as an image. Is there a way to post that inside the article instead of as an attachment? Thanks for the information to post from website but that is not what I am looking for. The primary article on Calcifediol and also the meta-analysis about Vitamin D for respiratory infections are both randomised clinical trials. They are not causual. In addition there is lot of causal data. Why are you StubbleJumper and Cigarbutt so hungup on causal studies part of my post ignoring the randomised clinical trials which are interventional trials?
-
How to insert an image inside a post? I am trying to post Vit D blood levels vs death rate plot for Covid 19. Thanks
-
That Vitamin D protects in respiratory infections is not a new information. My post above is for Covid 19. However there were lot of randomized clinical trials done for respiratory infections in general. Below is a reivew of such studies - published before Covid19 (December 2016). https://www.bmj.com/content/356/bmj.i6583 Systematic review and meta-analysis of individual participant data (IPD) from randomised controlled trials. Among those receiving daily or weekly vitamin D, protective effects were stronger in those with baseline 25-hydroxyvitamin D levels <25 nmol/L (adjusted odds ratio 0.30, 0.17 to 0.53) than in those with baseline 25-hydroxyvitamin D levels ≥25 nmol/L (adjusted odds ratio 0.75, 0.60 to 0.95; P for interaction=0.006). Vitamin D did not influence the proportion of participants experiencing at least one serious adverse event (adjusted odds ratio 0.98, 0.80 to 1.20, P=0.83). The body of evidence contributing to these analyses was assessed as being of high quality. Conclusions Vitamin D supplementation was safe and it protected against acute respiratory tract infection overall. Patients who were very vitamin D deficient and those not receiving bolus doses experienced the most benefit. ......................... I understand Odds ratio 1.0 means no effect. Odds ratio of 0.3 in patients with baseline 25-hydroxyvitamin D levels <25 nmol/L by administration of Vitamin D3, means 70% people got protected from respiratory disease. Note: Emphasis in bold added. Not medical advise. Consult your physician
-
tng. That study in Spain is a randomized clinical trial between 25OH Vit D vs standard of care (RCT, supposedly the only gold standard of clinical research) https://www.sciencedirect.com/science/article/pii/S0960076020302764 Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study” Design: Parallel pilot randomized open label, double-masked clinical trial. Participants: 76 consecutive patients hospitalized with COVID-19 infection, clinical picture of acute respiratory infection, confirmed by a radiographic pattern of viral pneumonia and by a positive SARS-CoV-2 PCR with CURB65 severity scale (recommending hospital admission in case of total score > 1). Even though they did not provide the incoming patients blood Vitamin D levels there are now many studies showing more serious patients have disproportionately Vitamin D deficiency. Below is one such study: https://www.medpagetoday.com/meetingcoverage/asbmr/88586 At the time of hospital admission, 25(OH)D levels were lower in the severely symptomatic group, at 18.2 ng/mL, than in the mildly symptomatic group, at 30.3 ng/mL, and in controls, at 25.4 ng/mL (P<0.0001 for both comparisons). So both from Causal relationship (more severe patients had lower Vitamin D) and now the Spanish showed one can give 25OH Vitamin D (Calcifediol) upon hospitalization with already pneumonia in radiological patterns and reduced the ICU admission by 95% compared to standard of care in a randomized clinical trial. Once we have randomized clinical trial with such result, supported by other causual relationships, I am not sure why many of you are questioning this? Should they repeat the clinical trial with more patients to confirm? Yes, absolutely. But it is also difficult to conduct such a study now. Who will volunteer not to take Vitamin D with such result already available?
-
https://www.businessinsider.com.au/fauci-takes-recommends-vitamin-d-and-c-supplements-immunity-boost-2020-9 Dr. Fauci says he takes vitamin D and C supplements and that they can lessen 'your susceptibility to infection' “If you’re deficient in vitamin D, that does have an impact on your susceptibility to infection. I would not mind recommending, and I do it myself, taking vitamin D supplements,” he said. “The other vitamin that people take is vitamin C because it’s a good antioxidant, so if people want to take a gram or so of vitamin C, that would be fine.”
-
On this, I don't disagree. I disagree that Herd immunity is the only way even without Vaccine. There are many ways to mitigate the virus transmission and its effects that are not being pursued. They include ventilation, drugs like HCQ+Zinc, Ivermectin, other small pharma drugs even with successful RCTs and Vitamin D. However, I want to focus on Vitamin D in this post. https://chrismasterjohnphd.com/covid-19/finally-confirmed-vitamin-d-nearly-abolishes-icu-risk-in-covid-19 Finally Confirmed! Vitamin D Nearly Abolishes ICU Risk in COVID-19 The above article is referring to a RCT done using Vitamin D metabolite from liver, Calcifediol (the form that they test in blood for Vitamin D levels). I understand they used this as it takes several days for Vitamin D to be converted into Calcifediol by liver and hence this form was used in hospital patients for treatment. The results were amazing. "To account for all of these differences, they adjusted for them statistically. In the adjusted model, vitamin D still reduced the odds of ICU admission by 97%, with the 95% confidence interval ranging from a 75% to a 99.7% reduction in the odds." We can presume a reduced ICU admission by 97% also would result in similar reduction in deaths. As the article points out this is not first time such a result was observed: "These results are consistent with the first observational study on vitamin D, which found that 96% of severe and critical cases occurred at 25(OH)D under 30 ng/mL, whereas 97.5% of mild cases had 25(OH)D above 30 ng/mL." There are also studies showing substantial decrease of infection with Vitamin D. A recent Univ. of Chicago study showed: https://www.upi.com/Health_News/2020/09/03/Vitamin-D-deficiency-raises-COVID-19-infection-risk-by-77-study-finds/7001599139929/ Vitamin D deficiency raises COVID-19 infection risk by 77%, study finds Why is this so? There are lot of articles talking about T-Cell based crossimmunity from other Coronaviruses for Covid-19. However there is research showing adequate Vitamin D levels are critical for T Cell immunity to function. Its referred as a on & off switch. With Vitamin D deficiency, the T Cell immunity will simply shut off. Here is one reference: https://www.sciencedaily.com/releases/2010/03/100307215534.htm Scientists have found that vitamin D is crucial to activating our immune defenses and that without sufficient intake of the vitamin - the killer cells of the immune system -- T cells -- will not be able to react to and fight off serious infections in the body. The research team found that T cells first search for vitamin D in order to activate and if they cannot find enough of it will not complete the activation process. Note: Emphasis in bold added