Investor20
-
Posts
518 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Everything posted by Investor20
-
I'm going to go with this one, rather than finding random permutations of doses of Hydroxychloroquine and other substances. "Oh, what about Hydroxychloroquine and Vitamin C? What about with Vitamin D? And water? And potatoes? And fire ants! Nobody's tried fire ants yet! Why can't you show me a study with fire ants!" I cannot find any details about patients given the medicine. If you have it please share. There are broadly two sets of data/claims 1) When given very early, even prophylactically HCQ alone works. That is the contention of Ford Health System why for them it worked. 2) NYU Grossman study said HCQ+Zinc+Azithromycin worked but not without Zinc. Many doctors say HCQ works by increasing availability of Zinc inside the cells where virus resides. Even with Zinc, NYU said it worked early and not later in disease progression. The Zelenko group from NY gives it very early, in a primary care physician and claims that it needs to be given even before they get the test result because by the time test results come and hospitalization, the virus has spread too much. The ICMR in India published studies prophylactically with only 400 mg once per week and showed decreased number of healthcare workers getting infected after several weeks of administration. https://www.indiatoday.in/india/story/4-hydroxychloroquine-hcq-doses-coronavirus-healthcare-workers-icmr-1684112-2020-06-01 4 or more hydroxychloroquine doses reduced risk of coronavirus in healthcare workers: ICMR study So besides your sarcastic statements, without knowing which patients are given the medicine such as oxygen levels and without any study with HCQ+Zinc, how can you conclude it doesnt work?
-
Sure, I can help you with that. The IV drug might provide some benefit, while random trials of the generic drug indicate it provides no benefit. Can you show me a randomized clinical study of Hydroxychloroquine of about 400 mg per day (approved dosage already for other diseases by FDA) for 5 -14 days. Preferably with Zinc. Given early in the infection. Can you cite me one? This is the dosage shown to be successful in restrospective studies, for exampe NYU grossman study given below. https://www.medrxiv.org/content/10.1101/2020.05.02.20080036v1.full.pdf Patients were categorized based on their exposure to hydroxychloroquine (400 mg load followed by 200 mg twice daily for five days) and azithromycin (500 mg once daily) alone or with zinc sulfate (220 mg capsule containing 50 mg elemental zinc twice daily for five days) as treatment in addition to standard supportive care.
-
NIH halts clinical trial of hydroxychloroquine https://www.nih.gov/news-events/news-releases/nih-halts-clinical-trial-hydroxychloroquine Yes and they wont test it and keep saying no randomized clinical studies available for HCQ, while HCQ is a tablet and generic and is available very cheap - essentially free. Meanwhile for Remedesivir which is expensive and given by IV which requires hospitalization, WHO and Dr. Fauci prioritized and did clinical studies already. So lets look at these study results https://www.gilead.com/news-and-press/press-room/press-releases/2020/6/gilead-announces-results-from-phase-3-trial-of-remdesivir-in-patients-with-moderate-covid-19 Gilead Announces Results From Phase 3 Trial of Remdesivir in Patients With Moderate COVID-19 In addition, non-statistically significant increases in clinical worsening or death were observed in the standard of care only group compared with the remdesivir groups. https://www.healthline.com/health-news/what-to-know-about-potential-covid-19-treatment-remdesivir Study sub-investigator Dr. Robert M. Grossberg, an associate professor of medicine at Albert Einstein College of Medicine and an infectious disease specialist at Montefiore Health System, said the results of this trial are “preliminary, but very promising.” “This was a well-designed study that proved that an antiviral drug could improve outcomes in patients with moderate to severe COVID-19,” he said. As for whether it keeps people from dying, he said the study “suggested that there might be a mortality benefit, but that wasn’t quite proven yet.” In early June, Gilead announced that other data showed that people with moderate COVID-19 recovered more quickly when given the drug for 5 days, although the benefit was “modest.” A 10-day course of the drug also improved patient outcomes, but the change wasn’t statistically significant. Patients in this study were hospitalized but didn’t need mechanical ventilation. ............................................ Now, can someone explain to me why would WHO and government organizations prioritize an expensive IV drug that needs to be given in a hospital including 10 day IV courses over a tablet that is generic and so cheap that it is essentially free, that can be given at home for clinical studies?
-
I think we all should do some deep DD (as we do when investing) before posting on technical things like effectiveness of a treatment. Moreover, I really think these BS studies should not be published and will not be published in any reputed journal. There are plenty of substandard journals that exist where these show up and someone incompetent in the media picks it up. Here is why this is a total BS study - (a) This is an retrospective observational study, not a randomized double blind clinical trial which is the gold standard and has shown no effectiveness. (b) Look at Table 1 of this study (https://www.ijidonline.com/article/S1201-9712(20)30534-8/fulltext) - the age itself can explain the difference in mortality. The patients receiving hydroxychloroquine alone (median age = 53) were younger by 18 years on average than who received no treatment (median age = 71). We already know younger patients survive better than older ones. So the patients treated with hydroxychloroquine simply lived because they were younger. One couldn't have picked a worst retrospective dataset than this for the analysis. That is why they had propensity matched patients in table 3 and hazard ratio for such patients in table 4. Agreed that the best way to do is randomized controlled studies. Unfortunately none were done by the WHO or Fauci department. But this is not the only study. There are at least three more in US alone. https://www.ny1.com/nyc/all-boroughs/news/2020/05/12/nyu-study-looks-at-hydroxychloroquine-zinc-azithromycin-combo-on-decreasing-covid-19-deaths Researchers at NYU's Grossman School of Medicine found patients given the antimalarial drug hydroxychloroquine along with zinc sulphate and the antibiotic azithromycin were 44 percent less likely to die from the coronavirus. https://link.springer.com/article/10.1007/s11606-020-05983-z#citeas Risk Factors for Mortality in Patients with COVID-19 in New York City A total of 858 of 6493 (13.2%) patients in our total cohort died: 52/2785 (1.9%) ambulatory patients and 806/3708 (21.7%) hospitalized patients. Cox proportional hazard regression modeling showed an increased risk of in-hospital mortality associated with age older than 50 years (hazard ratio 2.34, CI 1.47–3.71), systolic blood pressure less than 90 mmHg (HR 1.38, CI 1.06–1.80), a respiratory rate greater than 24 per min (HR 1.43, CI 1.13–1.83), peripheral oxygen saturation less than 92% (HR 2.12, CI 1.56–2.88), estimated glomerular filtration rate less than 60 mL/min/1.73m2 (HR 1.80, CI 1.60–2.02), IL-6 greater than 100 pg/mL (HR 1.50, CI 1.12–2.03), D-dimer greater than 2 mcg/mL (HR 1.19, CI 1.02–1.39), and troponin greater than 0.03 ng/mL (HR 1.40, CI 1.23–1.62). Decreased risk of in-hospital mortality was associated with female sex (HR 0.84, CI 0.77–0.90), African American race (HR 0.78 CI 0.65–0.95), and hydroxychloroquine use (HR 0.53, CI 0.41–0.67). Conclusions Among patients with COVID-19, older age, male sex, hypotension, tachypnea, hypoxia, impaired renal function, elevated D-dimer, and elevated troponin were associated with increased in-hospital mortality and hydroxychloroquine use was associated with decreased in-hospital mortality. https://www.preprints.org/manuscript/202007.0025/v1 COVID-19 Outpatients – Early Risk-Stratified Treatment with Zinc Plus Low Dose Hydroxychloroquine and Azithromycin: A Retrospective Case Series Study Conclusions: Risk stratification-based treatment of COVID-19 outpatients as early as possible after symptom onset with the used triple therapy, including the combination of zinc with low dose hydroxychloroquine, was associated with significantly less hospitalizations and 5 times less all-cause deaths. I am agreeing with you that randomized controlled studies are needed. When four studies above have given 40-80% reduction in death rate, for a medication that is essentially free, it should be done immediately . Unfortunately is not done yet.
-
Study finds hydroxychloroquine helped coronavirus patients survive better "Our results do differ from some other studies," Zervos told a news conference. "What we think was important in ours ... is that patients were treated early. For hydroxychloroquine to have a benefit, it needs to begin before the patients begin to suffer some of the severe immune reactions that patients can have with Covid," he added. Dr. Marcus Zervos, division head of infectious disease for Henry Ford Health System, said 26% of those not given hydroxychloroquine died, compared to 13% of those who got the drug. The Henry Ford team wrote that 82% of their patients received hydroxychloroquine within the first 24 hours of admission, and 91% within the first 48 hours of admission. https://www.msn.com/en-us/health/health-news/study-finds-hydroxychloroquine-helped-coronavirus-patients-survive-better/ar-BB16hifu I posted before about this timing of administration of antivirals in this thread. Antivirals would be expected to work better when administered early in infection.
-
https://www.worldometers.info/coronavirus/country/sweden/ For Sweden from Mid April to now the cases doubled from about 500 to 1000 per day the deaths meanwhile went from 100 to less than 10 per day. Doubling cases per day gave raise to tenfold reduction in deaths. Yet they keep posting only the cases without deaths.
-
https://www.medrxiv.org/content/10.1101/2020.06.28.20142190v1 By the week ending April 19, the seroprevalence in the screening group reached 19.3% https://www.6sqft.com/new-york-covid-antibody-test-preliminary-results/ Today, Governor Cuomo released the results of the state’s second-phase COVID antibody test, which randomly surveyed 12,000 people between May 1 and June 13. When the survey commenced, 12.3% of New York residents tested positive, compared with 13.4% on Saturday. The new results are more telling, however, when it comes to disparities in New York City. Though overall there was only a 1.6% increase (19.9% to 21.6%) But there were lots of cases from NYC from mid April to June. The antibodies are same. Is the below correct then? https://abcnews.go.com/Health/covid-19-antibodies-fade-months-study/story?id=71406787 COVID-19 antibodies may fade in as little as 2 months, study says Inspite of the cases between Mid April to Mid June, the antibody numbers did not change in NYC because they are fading?
-
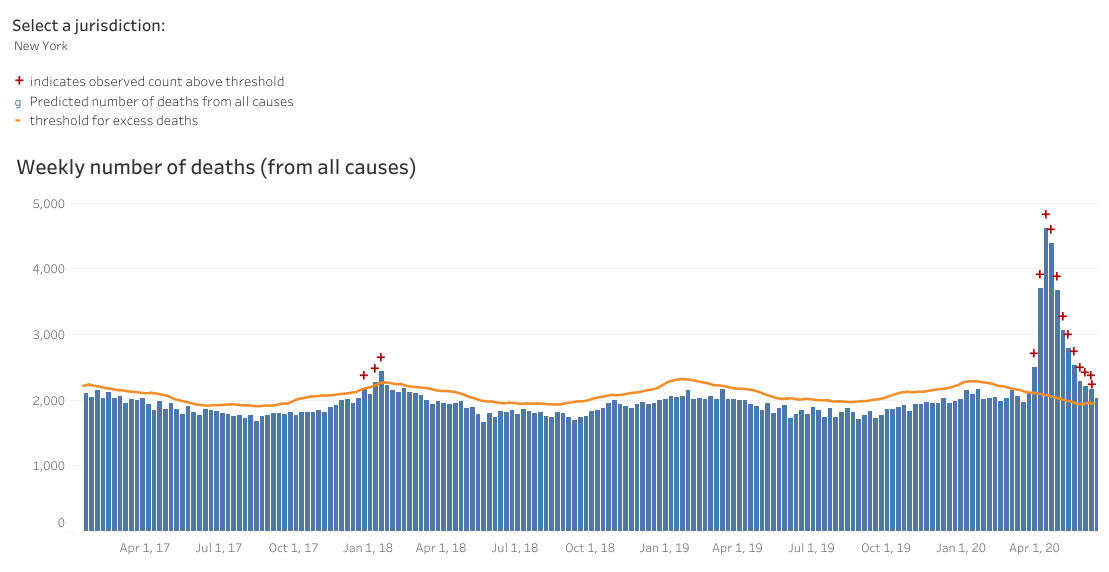
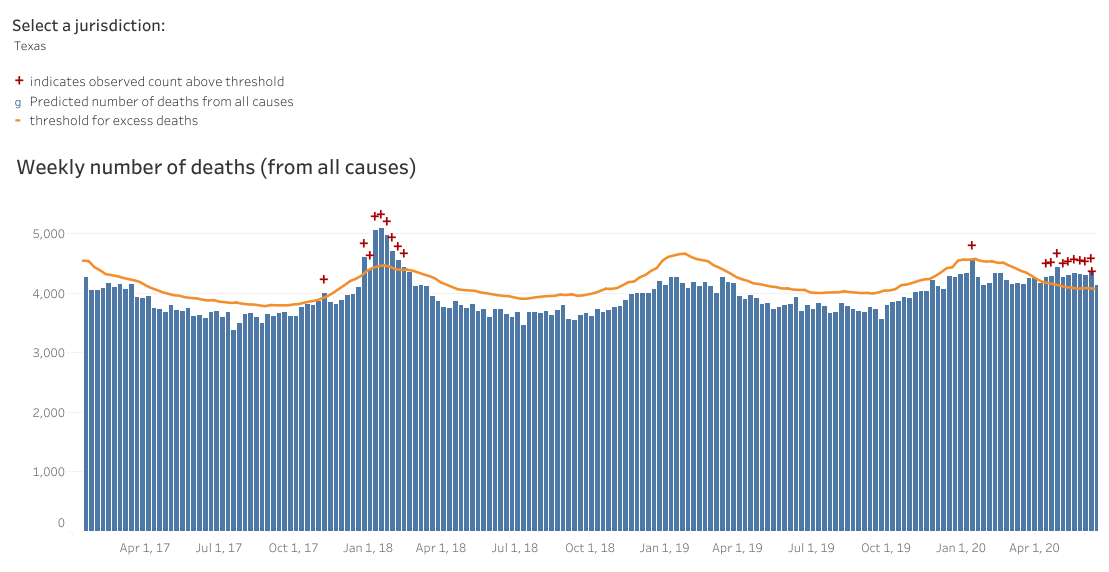
https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm Check out excess deaths by state. Florida, Arizona and Texas didnt have any more excess deaths than in 2018 winter. While NY, NJ have huge excess deaths. Plots for NY and Texas excess deaths shown below.

-
Pinning the problem on Cuomo is easy. Research indicates that infected travelers from New York transmitted nearly 65% of new coronavirus cases across the US, according to The New York Times. https://www.msn.com/en-in/news/world/people-who-traveled-from-new-york-across-the-us-in-early-march-caused-nearly-65-of-coronavirus-cases-in-the-rest-of-the-country-research-suggests/ar-BB13LgHK
-
With household infection, there probably isn't much you can do (you are probably infected by the time you realize that someone is sick). But in terms of office space or retail space, if "circulating air" is what is important, then air filters should also do a decent job because the good ones are rated to filter out particles as small as viruses. I have a theory that stuff like dust (which is all over the place indoors) could be a potential transmission vector as people are breathing it into their nose and breathing it back out and dust or pollen can fly around the air because they are "fluffy" and have large surface area and low density. This could be one of the reasons why masks seems to work in reducing infections even though they are ineffective at filtering out virus-sized particles in a laboratory. Virus infections could actually come from the virus riding on larger particles that we breathe deep into our lungs and breathe back out. Outdoors, the dust is dissipated pretty quickly so we don't keep re-breathing the same particles. Yeah, dust playing a role is possible, especially when the air is dry and electrostatic charges can play a huge role on how smaller particles like Viruses move in the air and attach themselves to other surfaces or particulars. The air circulation advice is great, but how many people or even business are going to be able to upgrade or change their air circulation systems (heating/ cooling) in a way that actually makes sense. Filtration System tend to be upstream, so upgrading the filters really won’t do anything if other expel in the same room add to the Virus load in the air. Depending on the restive location, air flow can even be detrimental as it can spread the Virus all over the in air. The idea situation would be to have the air flow like in a clean room, from the ceiling down and leaving through exhaust vents near the wall base all over in the room, but I don’t know any office that has this. I guess in some offices you could just vent though open windows , but that doesn’t work in high density multistory building where you can’t even open windows. In any case, I think the recent wave in infection at least partly was kicked off by Memorial Day parties and get together. Its a weak hypothesis thigh, based on the timing of the wave and the fact why mostly younger people are getting infected now. If correct , things are probably going to get worse after the 4th of July. I guess We will just have to see. First of all Japanese all ready have a law in place enforcing these requirements. If its so expensive and difficult, how did they get it running in few months? There is already research done with UV light and other systems. It is offered as a plumbing service even before Covid. The Church Trump gave used some ionization method that is installed inside the air duct. As per their website it costs 3000$. It is weird all media could think is criticize this because they used a Coronavirus surrogate for safety reasons to test the system instead of Covid-19. UV light had been used for long for TB control. Both TB and Coronavirus are sensitive to UV light. https://www.sciencedaily.com/releases/2009/03/090316201505.htm UV Light Cuts Spread Of Tuberculosis Introducing UVC lights could be a relatively low-cost measure, say the researchers. Currently, a typical UVC ceiling light costs around US$350 and replacement bulbs cost from US$25. The researchers are now working to develop more affordable US$100 units. https://plumblineservices.com/help-guides/how-much-does-it-cost-to-install-a-uv-light-for-my-hvac-system How Much Does It Cost to Install a UV Light for My HVAC System? the cost to install a UV light for an HVAC system can cost anywhere from $450 to $700+ in the Denver area. Depending only on cloth masks is not a great idea IMO. I posted one article by CIDRAP from Univ. of Minnesota saying no data exists to back cloth masks. Below is another article https://www.bmj.com/content/369/bmj.m1422 Covid-19: What is the evidence for cloth masks? But are they effective? Very little good quality research exists on the use of cloth masks, especially in non-medical settings. One randomised controlled clinical trial of cloth masks, published in BMJ Open in 2015, compared their effectiveness with that of medical masks worn by hospital healthcare workers.2 The study, involving the industry partner 3M (which makes medical masks), reported that healthcare workers “should not use cloth masks as protection against respiratory infection. Cloth masks resulted in significantly higher rates of infection than medical masks, and also performed worse than the control arm.” This is why I am saying CDC & Fauci are incompetent. Japanese did not do ground breaking research. They used already existing plumbing techniques that were available before Covid came up.
-
Here are the CDC guidelines for ventilation You really try hard to support incompetent people. "Consider", "recommendations"? No specific requirements for air flow per person. Why dont you use the same language for other guidelines too, of requesting Consideration of their recommendations? Why doesn't Cuomo come on TV and request consideration of his recommendation for shelter in place orders? Japanese are very clear with their 3Cs. They have a law in place to require certain amount of fresh air per person in an office. That gives confidence to employees to go to office. If protests are ok because they are outside, why not require employers to provide certain amount of ventilation and let people go to work? Why not tell how much fresh air or air which has been cleaned of virus is required so that employers can open their offices? Japanese had public transportation windows opened so that people can go to work. And most importantly they communicated these measures to the public so that both employers and employees are clear what environmental conditions they need to follow and are safe. Fauci and CDC could have told not only offices but shops how much air flow is required for shops to be opened. May be shop owners could have brought an exhaust fan and opened the shops? Where are those guidelines KCLarkin? Please dont keep saying outside for protests are ok, but we dont want to require offices to have specific ventilation scientifically determined so that people can go to work with confidence.
-
You are right, Japan even came up with this: According to this, clustering in Churches should definitely be avoided. In addition, in Japan and South Korea, it is so obvious and acceptable that everyone should be wearing a mask it wasn't even included in this poster. "Photos of the event taken inside the church showed the crowd shoulder to shoulder, with very few people appearing to wear masks.". Aren't you tired of your trolling? Yes this church is trying to avoid clusters by using technology to kill virus in ventilation ducts. Why criticize them for that? Why not WHO, Fauci, CDC, promote this way of reducing infections? You have not answered that. If protesters go out and and are very crowded for prolonged periods is ok, why not a church that ventilates and kills virus is not OK? I am personally not against wearing masks. In S. Korea everyone gets N95 masks. But, how well cloth masks work is debatable. See below article https://www.cidrap.umn.edu/news-perspective/2020/04/data-do-not-back-cloth-masks-limit-covid-19-experts-say Data do not back cloth masks to limit COVID-19, experts say In the paper, the National Academies' Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats said that, because no studies have been done on the effectiveness of cloth masks in preventing transmission of coronavirus to others, it is impossible to assess their benefits, if any.
-
Yes Indoor vs Outdoor there is a difference. But why won't the WHO, Fauci or CDC tell people to simulate conditions of outside by having good ventilation? Keep windows open. Have exhaust fans. Keep fresh air more in HVAC systems. Keep car ventilation on fresh. Try to avoid indoors as much as possible. Why not educate people on this? You can kill the virus inside the air systems by using UV light or HEPA filters or other engineering techniques. WHY??? Why won't they tell people? Afterall both S. Korea and Japan emphasize this ventilation a lot. WHO, Dr. Fauci or CDC don't know about this? Are they so ignorant? This Church below tried having a system that kills virus inside the air ducts. All the press could think of is criticize them. But the idea is fundamentally good. It will reduce the virus in air which is same what happens when you are outside. Why not say its a good idea? WHY? Why not tell people to do this more? https://www.nytimes.com/2020/06/23/us/politics/trump-arizona-church-covid.html Ahead of Trump Visit, Church Makes Unproven Claim of Virus-Killing Technology So what "unproven claim" they did? They tested with another Coronavirus that is safer to test with than the Covid-19 and said "kills 99.9 percent of Covid within 10 minute" instead of "kills 99.9 percent of Coronavirus within 10 minute". But what is the chance if one Coronavirus gets killed, Covid 19 also gets killed under same conditions?
-
https://www.yahoo.com/gma/covid-19-antibodies-may-fade-little-2-months-103252806--abc-news-topstories.html COVID-19 antibodies may fade in as little as 2 months, study says https://www.dailymail.co.uk/sciencetech/article-8331709/Oxford-coronavirus-vaccine-does-not-stop-infection-experts-warn.html Doubts raised over Oxford coronavirus vaccine after ALL of the monkeys that took part in the trial are found to have contracted the disease Oxford University vaccine has already been steam-rolled into human trials In the latest animal trials of the vaccine carried out on rhesus macaques, all six of the participating monkeys went on to catch the coronavirus. Dr William Haseltine, a former Harvard Medical School professor, revealed the monkeys who received the vaccine had the same amount of virus in their noses as the three non-vaccinated monkeys in the trial.
-
I haven't seen this study, but the obvious drawback is that prisons (aircraft carriers, cruise ships, etc) aren't representative populations. I'm not sure about the stats in that prison, but in Canada the majority of prisoners are young (20-40) males. So a CFR of 0.23% in that population would be consistent with a much higher IFR in the wider population. Did Ionnidis attempt to make this adjustment? Naively, I'd think that data would support an age-adjusted IFR closer to 1%. I'd also be reluctant to compare death rates between countries. According to CIA World Factbook, the U.S. has twice the obesity rate of Italy. In the U.S., I'd also be worried about the disparity in health care coverage. IFR is also not static. It depends on how stretched health care capacity is and the quality of treatment (which is evolving quickly). If you read Prof. Ioannidis (yes he is the few I would give that respect in this drama), he stated very clearly in his articles, he is adjusting the profile of the studies to the US demographic profile. Maybe I am dense, but I don’t see the Tousdale prison “study” in his Metaanalysis. Or is that in a different paper? I have not seen it in Prof. Ioannidis studies either. It is my search for cross checking. But he has covered other PCR studies to support himself. This is another https://www.npr.org/sections/coronavirus-live-updates/2020/04/20/838943211/73-of-inmates-at-an-ohio-prison-test-positive-for-coronavirus A state prison has become a hot spot of the COVID-19 outbreak in Ohio, with at least 1,828 confirmed cases among inmates — ..... The large cluster of cases was found through mass testing of everyone at the Marion Correctional Institution; 109 staff members were also positive. No COVID-19 deaths have been reported at the prison. "Because we are testing everyone — including those who are not showing symptoms — we are getting positive test results on individuals who otherwise would have never been tested because they were asymptomatic," the Ohio Department of Rehabilitation and Correction says.
-
I haven't seen this study, but the obvious drawback is that prisons (aircraft carriers, cruise ships, etc) aren't representative populations. I'm not sure about the stats in that prison, but in Canada the majority of prisoners are young (20-40) males. So a CFR of 0.23% in that population would be consistent with a much higher IFR in the wider population. Did Ionnidis attempt to make this adjustment? Naively, I'd think that data would support an age-adjusted IFR closer to 1%. I'd also be reluctant to compare death rates between countries. According to CIA World Factbook, the U.S. has twice the obesity rate of Italy. In the U.S., I'd also be worried about the disparity in health care coverage. IFR is also not static. It depends on how stretched health care capacity is and the quality of treatment (which is evolving quickly). If you read Prof. Ioannidis (yes he is the few I would give that respect in this drama), he stated very clearly in his articles, he is adjusting the profile of the studies to the US demographic profile.
-
Caution: Preprints are preliminary reports of work that have not been certified by peer review. They should not be relied on to guide clinical practice or health-related behavior and should not be reported in news media as established information. https://www.medrxiv.org/ John Ioannidis is the author of the discredited Santa Clara serology study. There were multiple issues with the study, including sampling bias, not adjusting for the sensitivity and specificity of the serology test, poststratification, and others. This new study aggregates his original study with a bunch of other seroprevalence studies with similar flaws, and gets the same as his original results....but with the same limitations. Perhaps the bottom line is best summed up by Nate Silver: When you look at locations with larger outbreaks, you see worse mortality rates. Why? Because if the false positive rate is 2%, then if the base rate of the population is 20% who have COVID, the error is only 10%, while if the base rate is 1%, it could be 200%. Serology surveys are used to tell us approximately what proportion of the population has had a disease, not typically to estimate the Infection Fatality Rate (IFR). There are numerous threads by good sources on Twitter from back in April on this by Trevor Bedford, Natalie Dean, PhD, and many others. One such thread here walks through a number of the limitations: A Columbia statistician named Andrew Gelman discusses the problems here: https://statmodeling.stat.columbia.edu/2020/04/19/fatal-flaws-in-stanford-study-of-coronavirus-prevalence/ Natalie Dean thread here: If you want an estimate based on less noisy data, you can look at the NYC population level deaths and you can calculate some back of the envelope estimates. Pretty clearly COVID hits older folks much harder, but I think the rates are higher than Ioannidis claims based on serology studies. https://www1.nyc.gov/site/doh/covid/covid-19-data.page Citywide, the death rate is .21% (that's of all people in NY, not just cases), with 75+ having a death rate of 1.57%, 65-74 0.63%, 45-64 0.19%, and 18-44 0.02%. That's on a population level, in a city with an estimated 25% prevalence, these numbers would have to be multiplied by 4 if you want to estimate the IFR, giving you approx 0.84% overall IFR, with subgroups 75+ 6.28%, 65-74 2.52%, 45-64 0.76%, 18-44 0.08%. Based on the data I've seen, those numbers look more realistic than Ioannidis. Like any good scientist, John Ioannidis is not basing it only on their testing in Santa Clara or even only the 20 other Seroprevalence testing (which should be enough). He also based it on PCR testing done on everyone (not just patients with symptoms) in Cruise Ships, people evacuated from Wuhan, Iceland, a small town in Italy, etc. For example, lets look at the Tennesse prisons where most prisoners were tested. As per below article, "is the third inmate to die after contracting the virus at the privately run Trousdale Turner Correctional Center" "Two weeks ago, Trousdale reported 1,299 inmates infected by the virus" That gives a CFR of (3/1299)*1000 = 0.23%. This is from PCR testing. Not Seroprevalence data. https://www.timesfreepress.com/news/breakingnews/story/2020/may/15/tennessee-prisons-report-fourth-inmate-death-virus-outbreak/523083/
-
I find that surprising since the CDC recommends getting the flu vaccine by the end of October each year. Then the number of flu cases rise afterwards. Because we all know that summer time respiratory diseases go down and winter they go up. Thats why they give flu vaccine in October. Nevertheless. Cases rising X amount after locking people down does not show that it was ineffective. For example, let's say one person in my household was just exposed on the morning the lockdown began. That person doesn't test positive for 10 more days, and then 10 more days after that a couple more people in the household come down with it. That's 20 days of lockdown and an explosion in cases within my household. Did you just accidentally make a case against lockdowns? ;) Yup. Eric just described how to get an explosion of cases. The data from NYC itself is clear. More crowded, more cases. People living in small houses, more cases. People going out such as transit and police, less cases. I take it you are being facetious. Intra-household spread is going to occur regardless of policy. No, I am not being facetious. See below. https://www.cnbc.com/2020/05/06/ny-gov-cuomo-says-its-shocking-most-new-coronavirus-hospitalizations-are-people-staying-home.html Cuomo says it’s ‘shocking’ most new coronavirus hospitalizations are people who had been staying home
-
Are cases starting to go down? People who propose lockdowns are the one who have to show cases and more importantly deaths are going up after lockdowns are stopped. Lockdowns have severe economic, psychological and medical negative consequences. Just in US 75000 people are estimated to have suicides because of lockdowns. UN warned that hundreds of thousands of children could die because of lockdown. Let alone millions who lose their jobs. People who propose lockdowns are those who have to show lockdowns are worth that price.
-
I find that surprising since the CDC recommends getting the flu vaccine by the end of October each year. Then the number of flu cases rise afterwards. Because we all know that summer time respiratory diseases go down and winter they go up. Thats why they give flu vaccine in October. Nevertheless. Cases rising X amount after locking people down does not show that it was ineffective. For example, let's say one person in my household was just exposed on the morning the lockdown began. That person doesn't test positive for 10 more days, and then 10 more days after that a couple more people in the household come down with it. That's 20 days of lockdown and an explosion in cases within my household. Did you just accidentally make a case against lockdowns? ;) Yup. Eric just described how to get an explosion of cases. The data from NYC itself is clear. More crowded, more cases. People living in small houses, more cases. People going out such as transit and police, less cases.
-
A company with hardly any technical background, with a person with background as Sci Fi writer as scientific expert and another with background as Adult entertainer as director of marketing. But such miniscule details doesn't matter. Its Lancet, peer reviewed and signed off by Harvard professor.
-
I find that surprising since the CDC recommends getting the flu vaccine by the end of October each year. Then the number of flu cases rise afterwards. Because we all know that summer time respiratory diseases go down and winter they go up. Thats why they give flu vaccine in October. Though everyone was fighting with me in March when I said cases will go down in summer. So they were modelling cases exponentially continuously going up without lockdown. But that is not correct. Cases will start going down in summer and an honest modelling will take that into account. But lockdown in March/April is a different beast. Normally they start going down for respiratory diseases by March/April.
-
https://vdata.nikkei.com/en/newsgraphics/coronavirus-economy/ Thanks. And it shows Japanese overall had much more mobility than New York. It is interesting Parks & Supermarkets activity did not go down much at all for Japan. The parks data shows Japanese were educated upfront about enclosed places. Japanese were going out to parks all through Feb-Jun, while New yorkers reduced going out to parks. When someone is outside at park, they are not at home - automatic social distancing.
-
Yes, this is why I called Gato's analysis the stupidest thing posted on this thread! Let's do this analysis for February. U.S. -> 1 death, no lockdown Canada -> 0 deaths, no lockdown Wuhan -> Thousands of deaths*, lockdown. Lockdowns are definitely correlated with deaths! But, I'm confident that Wuhan locked down BECAUSE of the outbreak. * numbers made up Lets take this further. Causation comes with timing. When did lockdown start in New York City? When did all the deaths come. Before or after? Well, most people die of the flu after the vaccine has been administered. Another correlation: most of the deaths came after Trump told us that he shut down the flights from China. And it all happened after Valentine's Day, so I'm wondering if all those Hallmark cards were involved. After Flu vaccine is given, number of cases of flu go down, not up. After lockdown did cases go down or up?
-
Yes, this is why I called Gato's analysis the stupidest thing posted on this thread! Let's do this analysis for February. U.S. -> 1 death, no lockdown Canada -> 0 deaths, no lockdown Wuhan -> Thousands of deaths*, lockdown. Lockdowns are definitely correlated with deaths! But, I'm confident that Wuhan locked down BECAUSE of the outbreak. * numbers made up Lets take this further. Causation comes with timing. When did lockdown start in New York City? When did all the deaths come. Before or after?